Therapy in Body Dysmorphic Disorder (BDD): What Actually Helps
 Body Dysmorphic Disorder (BDD) is not a cosmetic problem and not a problem of low confidence. It is a treatable psychiatric condition rooted in distorted perception, obsessive thinking, and maladaptive coping behaviours. While medication plays an important role, psychotherapy is the cornerstone of long-term recovery in BDD.
Body Dysmorphic Disorder (BDD) is not a cosmetic problem and not a problem of low confidence. It is a treatable psychiatric condition rooted in distorted perception, obsessive thinking, and maladaptive coping behaviours. While medication plays an important role, psychotherapy is the cornerstone of long-term recovery in BDD.
This article explains what therapy works in BDD, why it works, and what patients should realistically expect, especially in the Indian clinical context.
Why Therapy Is Essential in BDD
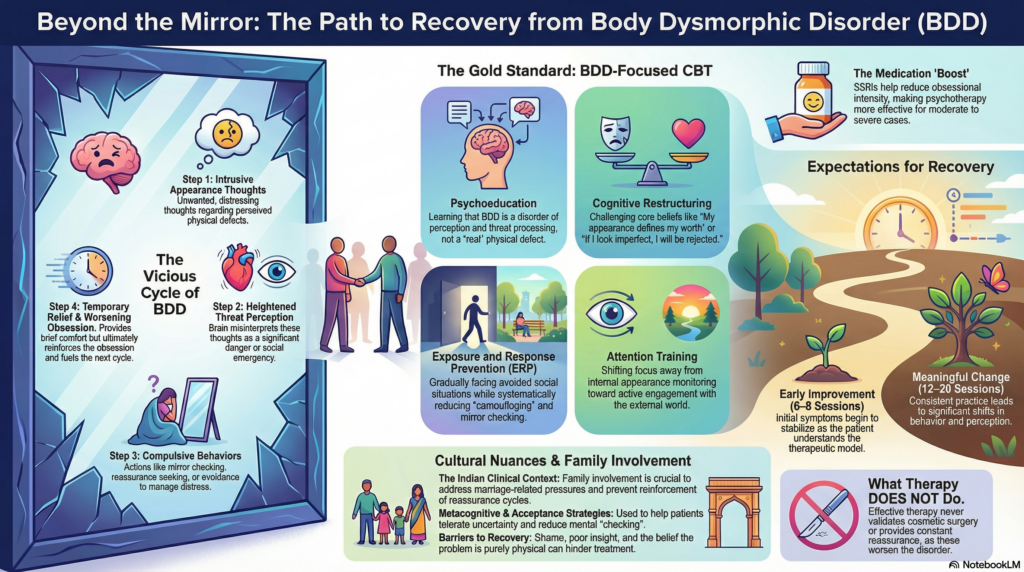
BDD is maintained by a vicious cycle:
-
Intrusive appearance-related thoughts
-
Heightened threat perception
-
Compulsive behaviours (mirror checking, reassurance seeking, avoidance)
-
Temporary relief followed by worsening obsession
Therapy targets this cycle directly.
Cosmetic reassurance does not.
Without therapy:
-
Insight often remains partial
-
Relapse risk stays high
-
Dependence on external reassurance continues
First-Line Psychotherapy: Cognitive Behaviour Therapy (CBT) for BDD
CBT is the most evidence-based psychotherapy for BDD and is recommended by international guidelines.
BDD-focused CBT differs from generic CBT.
Core Components of CBT in BDD
-
Psychoeducation
Patients learn that BDD is a disorder of perception and threat processing—not a real defect. -
Cognitive Restructuring
Therapy challenges beliefs such as:
-
“If I look imperfect, I will be rejected”
-
“My appearance defines my worth”
-
Exposure and Response Prevention (ERP)
Patients gradually:
-
Reduce mirror checking
-
Stop reassurance seeking
-
Face avoided situations without camouflaging
-
Attention Training
Shifting focus away from internal appearance monitoring to external engagement.
CBT does not aim to convince patients they “look fine”.
It helps the brain stop treating appearance as danger.
Insight-Oriented Work: When and Why It Helps
Many patients with BDD have poor or fluctuating insight. Some are convinced the defect is real, others intellectually doubt it but remain emotionally trapped.
Therapy helps by:
-
Improving insight gradually
-
Reducing rigidity of beliefs
-
Allowing emotional learning through experience, not reassurance
Direct confrontation of beliefs rarely works early.
Collaborative exploration does.
Role of Metacognitive and Acceptance-Based Approaches
In some patients, especially those with high rumination, metacognitive strategies are useful:
-
Reducing mental checking
-
Changing the relationship with thoughts
-
Learning not to engage with appearance-related worry
Acceptance-based techniques help patients:
-
Tolerate uncertainty
-
Reduce compulsive attempts to “fix” distress
-
Re-engage with life despite residual discomfort
Family Involvement in Therapy (Especially in India)
In the Indian context, family plays a major role in:
-
Reinforcing reassurance
-
Encouraging cosmetic solutions
-
Minimising psychological distress
Family psychoeducation helps by:
-
Reducing reassurance cycles
-
Addressing marriage-related pressures
-
Aligning expectations with recovery goals
Without family involvement, therapy progress is often slower.
What Therapy Does Not Do
Effective therapy for BDD does not:
-
Provide repeated reassurance about appearance
-
Validate cosmetic correction as a solution
-
Focus on self-esteem alone
-
Encourage excessive mirror exposure
These approaches unintentionally strengthen the disorder.
How Long Does Therapy Take in BDD?
BDD therapy is not instant.
-
Early improvement: 6–8 sessions
-
Meaningful change: 12–20 sessions
-
Severe or long-standing BDD: longer-term work
Progress is often non-linear, with periods of doubt and resistance. This is expected and manageable.
Therapy + Medication: A Powerful Combination
For moderate to severe BDD, therapy works best alongside medication, usually SSRIs at adequate doses.
Medication reduces:
-
Obsessional intensity
-
Emotional reactivity
Therapy then becomes more effective and tolerable.
Common Barriers to Therapy in BDD
-
Shame and fear of judgement
-
Belief that the problem is “physical”
-
Family pressure for cosmetic fixes
-
Poor insight
Addressing these barriers is part of therapy—not a prerequisite.
Key Takeaways
-
Therapy is central to recovery in BDD
-
CBT tailored for BDD is the gold standard
-
Cosmetic reassurance worsens outcomes
-
Family involvement improves success in India
-
Recovery focuses on function and freedom, not perfect appearance
BDD is treatable—but only when therapy addresses how the mind sees, not what the mirror shows.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Dr. Srinivas Rajkumar T is a Chennai-based psychiatrist with clinical expertise in obsessive–compulsive spectrum disorders, Body Dysmorphic Disorder, anxiety disorders, and mood disorders. His approach integrates evidence-based psychotherapy, psychopharmacology, and culturally informed psychoeducation, particularly for appearance-related psychiatric conditions.
📍 Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com
📞 +91-8595155808