Metacognitive Model of Anxiety
 Why do anxious thoughts persist even when people know their fears are exaggerated or irrational?
Why do anxious thoughts persist even when people know their fears are exaggerated or irrational?
Why does reassurance help briefly, only for worry to return stronger?
The metacognitive model of anxiety, developed by Adrian Wells, offers a powerful answer:
anxiety is not maintained by what we think, but by how we relate to our thoughts.
This model forms the backbone of Metacognitive Therapy (MCT) and represents a significant shift from traditional cognitive approaches. Instead of analysing the content of thoughts, it examines the processes that keep the mind locked in worry and threat monitoring.
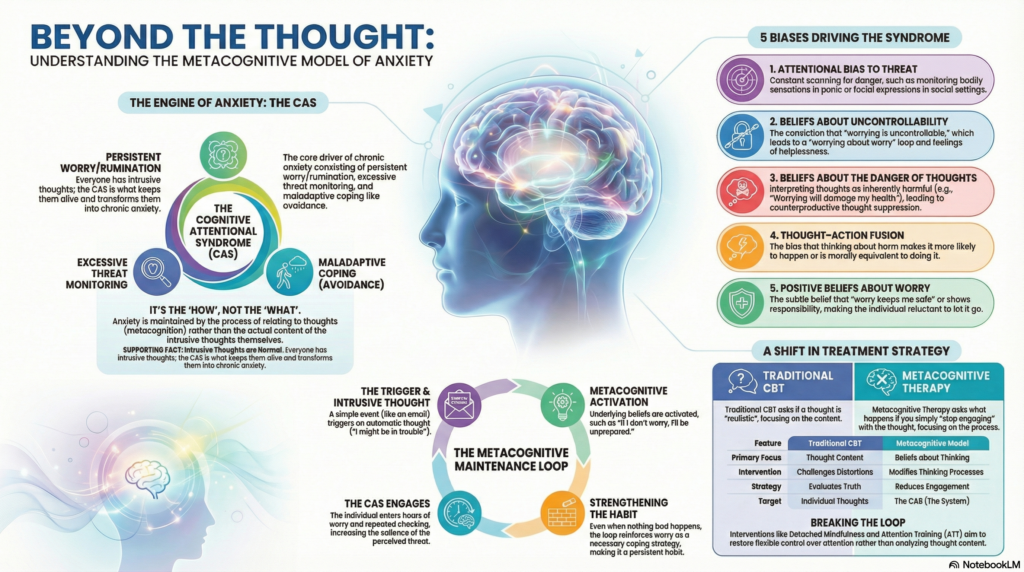
The Core Idea: Anxiety Is Maintained by the Cognitive Attentional Syndrome (CAS)
According to the metacognitive model, anxiety becomes chronic because of a self-perpetuating pattern called the Cognitive Attentional Syndrome (CAS).
The CAS consists of:
• Persistent worry or rumination
• Excessive monitoring for threat
• Maladaptive coping strategies (avoidance, reassurance seeking, checking)
• Dysfunctional metacognitive beliefs
Crucially, it is not the initial intrusive thought that causes ongoing anxiety. Intrusive thoughts are universal and normal.
It is the CAS, activated by metacognitive beliefs, that keeps anxiety alive.
Cognitive Biases in the Metacognitive Model
Traditional CBT focuses on distortions in thought content (e.g., catastrophising, overgeneralisation).
The metacognitive model instead highlights biases in processing style, control, and interpretation of thinking itself.
These biases determine how much attention we give thoughts and how seriously we take them.
1. Attentional Bias to Threat
This bias involves selective and sustained monitoring for danger.
Common examples include:
• Scanning bodily sensations in panic disorder
• Monitoring facial expressions in social anxiety
• Checking for intrusive thoughts in OCD
The underlying belief becomes:
“Threat is everywhere, and I must stay alert.”
As attention narrows, even neutral sensations or thoughts acquire a sense of danger. The mind learns to treat harmless stimuli as meaningful threats.
2. Beliefs About Uncontrollability of Worry
A central metacognitive belief is:
“My worrying is uncontrollable.”
This belief produces a paradoxical effect. People begin to worry about worrying.
A vicious loop develops:
Worry → fear of losing control → intensified worry
The individual no longer sees worry as a choice, but as an unstoppable mental force—fueling helplessness and anxiety.
3. Beliefs About the Danger of Thoughts
Here, thoughts are interpreted as inherently dangerous.
Common beliefs include:
• “If I think this, something bad might happen”
• “Worrying will damage my health”
• “These thoughts mean I’m losing control of my mind”
These beliefs drive coping strategies such as:
• Thought suppression
• Mental checking
• Reassurance seeking
• Neutralising rituals
Ironically, these strategies increase the frequency and intensity of intrusive thoughts, reinforcing the original fear.
4. Thought–Action Fusion
Especially prominent in OCD and health anxiety, this bias takes two forms:
• Likelihood fusion: thinking about harm increases its probability
• Moral fusion: thinking something bad is morally equivalent to doing it
The result is heightened vigilance and compulsive neutralisation, keeping attention locked onto threat.
5. Positive Beliefs About Worry
This bias is subtle and often missed—but it is vital.
Typical beliefs include:
• “Worry keeps me safe”
• “If I stop worrying, I’ll be unprepared”
• “Worry shows I’m responsible”
As long as worry is seen as useful, the CAS remains active. The individual is ambivalent about letting go of worry, even while suffering from it.
How the Metacognitive Model Differs from Traditional CBT
Traditional CBT asks:
“Is this thought accurate or realistic?”
The metacognitive model asks:
“What happens if you stop engaging with this thought?”
| Traditional CBT | Metacognitive Model |
|---|---|
| Focus on thought content | Focus on beliefs about thinking |
| Challenges distortions | Modifies thinking processes |
| Evaluates truth | Reduces engagement |
| Targets individual thoughts | Targets the CAS |
The goal is not to replace negative thoughts with positive ones, but to disengage from unhelpful thinking patterns altogether.
The Metacognitive Maintenance Loop
A typical anxiety cycle unfolds as follows:
Trigger
→ Intrusive thought
→ Metacognitive belief activated
→ Worry, monitoring, suppression
→ Increased salience of threat
→ More intrusive thoughts
→ Strengthened belief in uncontrollability
Over time, the person becomes trapped in this loop—not because of danger, but because of how the mind responds to thoughts.
Clinical Implications
Metacognitive Therapy aims to switch off the CAS, rather than analyse every thought.
Key interventions include:
• Detached mindfulness (observing thoughts without engagement)
• Attention Training Technique (ATT)
• Postponement of worry
• Modifying beliefs about uncontrollability
• Reducing threat monitoring
The objective is not to eliminate intrusive thoughts—an impossible task—but to restore flexible control over attention and thinking.
Example Formulation: Generalised Anxiety Disorder
Trigger: Email from boss
Thought: “I might be in trouble”
Metacognitive belief: “If I don’t worry, I’ll miss something important”
CAS: Hours of worry, repeated inbox checking
Outcome: Heightened anxiety and reinforcement of worry as a coping strategy
Nothing catastrophic occurs, yet worry is strengthened as a habit.
Why This Model Matters
The metacognitive model explains why reassurance, insight, and logical arguments often fail in anxiety disorders.
It shifts therapy away from endless thought-challenging toward changing how the mind relates to thinking itself.
In doing so, it offers a clearer, more efficient path out of chronic anxiety.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808