rTMS for Auditory Hallucinations: A Practical, Evidence-Based Perspective
 Auditory verbal hallucinations (AVH) remain one of the most distressing symptoms of schizophrenia and related psychotic disorders. While antipsychotic medications are the cornerstone of treatment, a significant subgroup of patients continue to experience persistent voices despite adequate pharmacological trials.
Auditory verbal hallucinations (AVH) remain one of the most distressing symptoms of schizophrenia and related psychotic disorders. While antipsychotic medications are the cornerstone of treatment, a significant subgroup of patients continue to experience persistent voices despite adequate pharmacological trials.
Repetitive Transcranial Magnetic Stimulation (rTMS) has emerged as an evidence-supported adjunctive intervention for such treatment-resistant auditory hallucinations. Though not a cure, it offers a neurobiologically informed way to modulate the brain circuits implicated in hallucination generation.
The Neurobiology Behind Voices
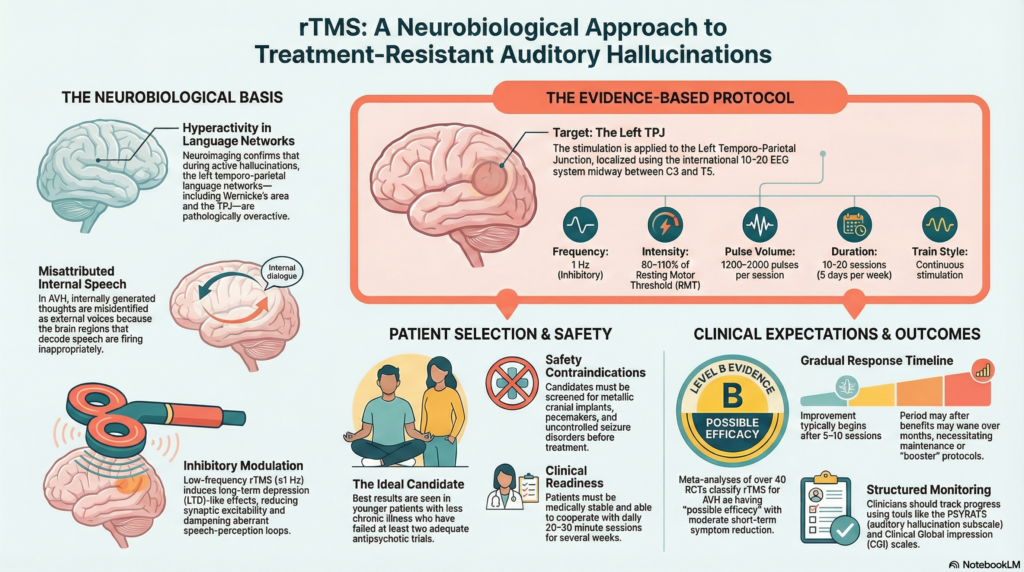
Neuroimaging studies over the last two decades have been remarkably consistent. During active auditory hallucinations, there is hyperactivity in left temporo-parietal language networks, especially regions involved in speech perception and comprehension.
Key areas implicated include:
-
Posterior superior temporal gyrus
-
Temporo-parietal junction (TPJ)
-
Wernicke’s area
These regions normally help us decode external speech. In AVH, internally generated speech appears to be misattributed as external, leading to the subjective experience of “hearing voices.”
Low-frequency rTMS (≤1 Hz) reduces cortical excitability. Applied to the left TPJ, it is thought to inhibit pathological overactivity in language perception circuits, thereby reducing hallucination frequency or distress.
This pathophysiological rationale is one of the strongest aspects of rTMS for AVH—it is not arbitrary stimulation, but targeted circuit modulation.
Where Exactly Is rTMS Applied?
The Target: Left Temporo-Parietal Junction (TPJ)
In routine clinical practice, the left TPJ is localized using the international 10–20 EEG system:
-
Positioned approximately midway between C3 and T5
-
Slightly posterior to classical Wernicke’s area
-
Neuronavigation, when available, improves accuracy but is not mandatory
This target corresponds well with functional imaging findings from AVH studies and is widely used in clinical trials and workshops.
Evidence-Based rTMS Protocol for AVH
Based on international guidelines (notably Lefaucheur et al.) and cumulative clinical trial data, the standard protocol is as follows:
| Parameter | Typical Setting |
|---|---|
| Frequency | 1 Hz (low frequency, inhibitory) |
| Target | Left TPJ |
| Intensity | 80–110% of Resting Motor Threshold (RMT) |
| Pulses per session | 1200–2000 |
| Sessions | 10–20, usually 5 sessions per week |
| Train | Continuous 1 Hz stimulation |
This protocol has been the most consistently studied and remains the clinical reference point.
How Strong Is the Evidence?
Meta-analyses and systematic reviews have evaluated over 40 randomized controlled trials examining rTMS for auditory hallucinations.
What the data show:
-
Moderate short-term reduction in hallucination severity
-
Best response in:
-
Younger patients
-
Less chronic illness
-
Prominent, treatment-resistant AVH
-
Limitations are equally important to acknowledge:
-
Benefits often wane over weeks to months
-
Maintenance or booster protocols are not yet standardized
-
Effect sizes are modest rather than dramatic
Current guideline position classifies rTMS for AVH as having “possible efficacy” (Level B)—strong enough to justify clinical use, but not yet definitive.
Selecting the Right Patient
rTMS works best when offered to carefully selected patients.
Ideal candidates typically have:
-
Persistent AVH despite at least two adequate antipsychotic trials
-
Medical and neurological stability
-
No metallic cranial implants or pacemakers
-
No uncontrolled seizure disorder
-
Ability to cooperate with daily sessions
Thorough safety screening and expectation-setting are essential before initiation.
When Standard Protocols Don’t Work
Not all patients respond to left TPJ 1 Hz stimulation. In partial or non-responders, several strategies are under exploration:
-
Bilateral TPJ stimulation
-
Theta burst stimulation (experimental)
-
High-frequency left DLPFC stimulation (especially if negative symptoms coexist)
-
Combined TPJ + DLPFC protocols (research settings)
These approaches remain investigational and should be used cautiously, ideally within structured programs.
Practical Clinical Considerations
Before starting rTMS:
-
Determine RMT carefully
-
Use hearing protection
-
Explain realistic outcomes
Patients should understand:
-
Improvement often begins after 5–10 sessions
-
Benefits are gradual and variable
-
Booster sessions may be needed in some cases
Monitoring response using structured tools improves clinical decision-making:
-
PSYRATS (auditory hallucination subscale)
-
Clinical Global Impression (CGI)
-
Simple frequency and distress ratings
What Is rTMS Doing at a Cellular Level?
Low-frequency rTMS induces long-term depression (LTD)-like effects, reducing synaptic excitability in overactive cortical circuits.
In AVH, this likely translates into:
-
Reduced gamma synchrony in language networks
-
Dampening of aberrant speech-perception loops
-
Improved discrimination between internal and external speech
These mechanisms align neatly with modern models of cortical excitability and predictive processing.
Key Take-Home Points
-
Target: Left temporo-parietal junction
-
Frequency: 1 Hz
-
Intensity: 80–110% RMT
-
Sessions: 10–20
-
Evidence: Moderate, short-term benefit
-
Best suited for: Treatment-resistant auditory hallucinations
rTMS should be seen not as a replacement for medication, but as a neurobiologically informed adjunct—especially valuable when conventional approaches plateau.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808