Clinical Applications of the 10–20 System: From Diagnosis to Brain Stimulation
 Introduction
Introduction
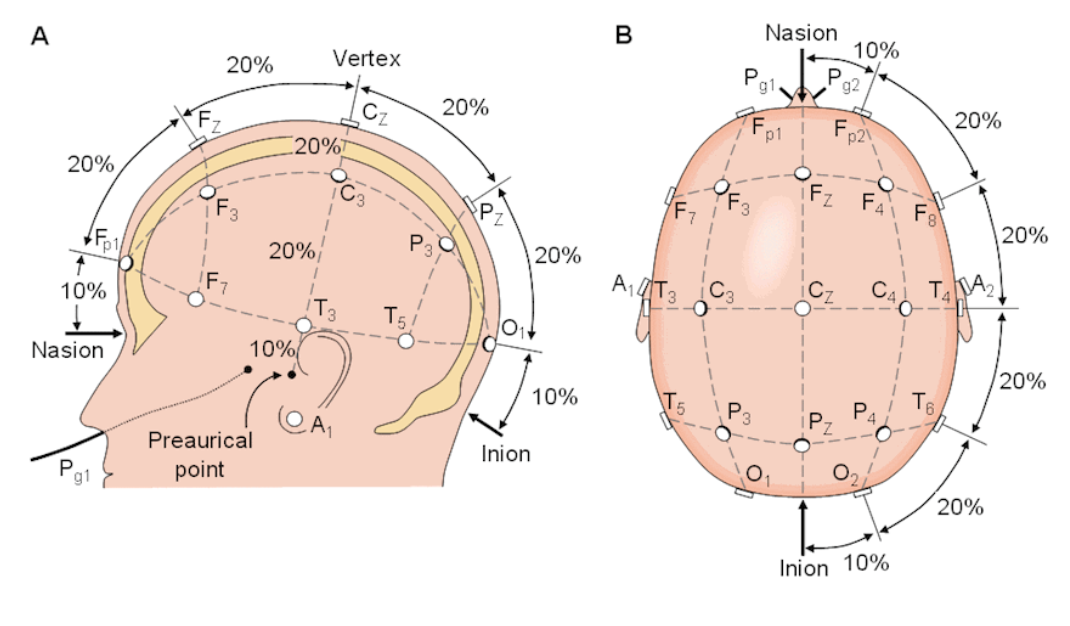
The International 10–20 system started as a method for standardized EEG electrode placement, but over the decades, it has become a cornerstone in many areas of clinical neuroscience.
From diagnosing epilepsy to delivering targeted brain stimulation for depression, this simple coordinate system allows clinicians across the globe to speak the same anatomical language.
Whether in a high-tech neuromodulation lab or a rural EEG clinic, the 10–20 system ensures reliability, reproducibility, and clinical relevance.
1. In Neurology: EEG Diagnostics
Epilepsy Localization
-
Temporal lobe epilepsy → Abnormalities at T3/T7 or T4/T8.
-
Frontal lobe epilepsy → F3/F4 or F7/F8 involvement.
-
Occipital seizures → O1/O2 discharges.
Precise electrode placement improves localisation, guiding surgical decisions.
Encephalopathy
-
Diffuse slowing patterns captured across multiple electrode sites.
-
Triphasic waves often prominent in frontal leads.
Coma and Prognostication
-
Reactivity testing across the 10–20 map can predict recovery chances.
-
Brain death confirmation includes assessing EEG silence across standard positions.
Sleep Medicine
-
Occipital alpha attenuation, frontal slow waves, and central sleep spindles rely on correct electrode placement.
2. In Psychiatry: rTMS & Neuromodulation
Depression
-
Left dorsolateral prefrontal cortex (F3) targeted with high-frequency (10 Hz) rTMS.
-
Improves prefrontal–limbic network regulation.
OCD
-
Supplementary motor area (near FCz) targeted with low-frequency (1 Hz) to reduce hyperactivity.
PTSD & Anxiety
-
Right DLPFC (F4) targeted to modulate fear circuits.
Addiction
-
Medial prefrontal and dorsolateral prefrontal targets modulated to reduce craving.
3. In Rehabilitation Medicine
Stroke Recovery
-
Motor cortex mapping (C3/C4) guides rTMS for motor recovery.
-
Contralesional inhibition or ipsilesional facilitation protocols depend on lesion side.
Motor Threshold Determination
-
C3/C4 used to identify motor hotspot for individualized dosing in rTMS.
4. In Neuropsychology & Research
Cognitive Testing
-
EEG at specific 10–20 positions during memory or attention tasks helps map functional activation.
Brain–Computer Interfaces (BCIs)
-
Sensorimotor rhythm BCIs use central electrodes (C3, Cz, C4) to decode motor intentions.
Neurofeedback
-
Training alpha at occipital sites (O1/O2) or beta at frontal sites (F3/F4) to improve cognitive or emotional states.
5. Emerging Clinical Applications
Closed-Loop Neuromodulation
-
Combining EEG and rTMS using 10–20 landmarks for real-time feedback-based targeting.
Portable EEG for Telemedicine
-
Dry-electrode headsets often use simplified 10–20 positions for home monitoring.
Hybrid EEG–fNIRS Systems
-
fNIRS optodes are aligned to 10–20 coordinates for multimodal brain mapping.
Advantages of Using the 10–20 System in Clinical Work
-
Universality → Standardised communication between clinicians worldwide.
-
Accessibility → No expensive imaging required.
-
Versatility → Works for diagnosis, treatment, research, and monitoring.
-
Evidence-based → Validated in thousands of clinical studies.
Limitations in Clinical Practice
-
Inter-individual variability in skull–brain mapping.
-
Limited resolution for deep brain structures.
-
Not as precise as MRI-based neuronavigation for small or atypical targets.
Closing Thoughts
The 10–20 system may have been born in the EEG lab, but its utility extends far beyond.
In the hands of a skilled clinician, it becomes a map for diagnosis, a guide for treatment, and a framework for research — all without the need for high-end equipment.
In an age of precision medicine, the 10–20 system remains a bedrock principle, ensuring that wherever you are in the world, “F3” means the same place — and the patient in front of you gets care that’s accurate, consistent, and grounded in decades of science.