Xanomeline–Trospium: A New Dopamine-Sparing Direction in Schizophrenia Treatment
 For more than seventy years, the treatment of schizophrenia has largely revolved around one central idea: reduce dopamine D2 receptor activity. This approach has helped millions of patients with hallucinations, delusions, suspiciousness and thought disorganisation. But it has also left important gaps. Many patients continue to struggle with motivation, emotional expression, social functioning, cognition, planning, attention, memory and day-to-day independence even when positive symptoms improve.
For more than seventy years, the treatment of schizophrenia has largely revolved around one central idea: reduce dopamine D2 receptor activity. This approach has helped millions of patients with hallucinations, delusions, suspiciousness and thought disorganisation. But it has also left important gaps. Many patients continue to struggle with motivation, emotional expression, social functioning, cognition, planning, attention, memory and day-to-day independence even when positive symptoms improve.
This is why the approval of xanomeline–trospium is important. In September 2024, the U.S. FDA approved this oral medication for adults with schizophrenia, describing it as the first antipsychotic approved for schizophrenia that targets cholinergic receptors rather than dopamine receptors.
Why this drug is scientifically interesting
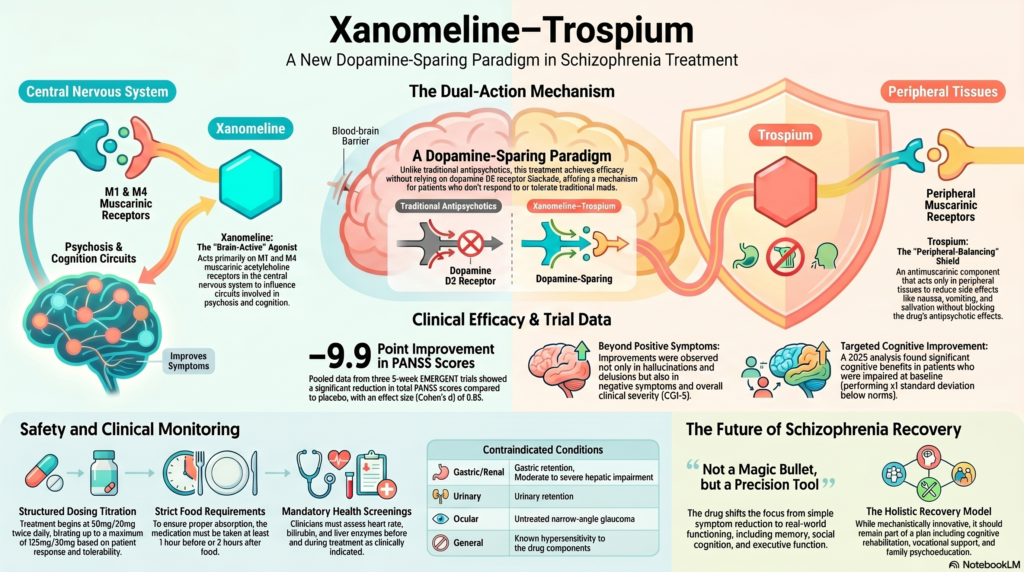
Xanomeline–trospium is not simply “another antipsychotic.” It represents a different pharmacological strategy. The xanomeline component acts mainly through muscarinic acetylcholine receptors, especially M1 and M4 receptor activity in the central nervous system. The official prescribing information states that xanomeline’s efficacy is thought to be due to agonist activity at M1 and M4 muscarinic acetylcholine receptors, while trospium is a muscarinic antagonist acting primarily in peripheral tissues.
In simpler terms, xanomeline is the “brain-active” part intended to influence circuits involved in psychosis and cognition. Trospium is added to reduce unwanted peripheral cholinergic effects such as nausea, vomiting, sweating, salivation, abdominal cramping and diarrhoea. Trospium is not the antipsychotic component; it is the balancing component.
This is clinically elegant because it tries to use the therapeutic potential of muscarinic stimulation while limiting the body-level side effects that made earlier muscarinic drugs difficult to tolerate.
Why moving beyond dopamine matters
Dopamine blockade remains powerful, but it is not a complete answer. Traditional antipsychotics are often effective for positive symptoms, but cognitive and negative symptoms remain major drivers of disability. The Cambridge Cognition CIAS report highlights that nearly all available schizophrenia treatments have been centred on dopamine D2 blockade and that these medications have minimal effects on negative and cognitive symptoms.
This matters because real-world recovery in schizophrenia is not only about reducing hallucinations or delusions. It is also about whether a person can study, work, manage relationships, plan the day, interpret social situations, remember tasks, and rebuild a meaningful life.
What did the clinical trials show?
Across pooled data from three 5-week randomized, double-blind, placebo-controlled EMERGENT trials, xanomeline–trospium significantly improved PANSS total scores compared with placebo at week 5. The pooled least-squares mean difference was –9.9 points, with a Cohen’s d effect size of 0.65, and improvements were also seen in PANSS positive, negative and CGI-Severity scores.
This is important for two reasons. First, the improvement was not restricted only to positive symptoms. Second, the signal appeared across multiple trials, strengthening confidence that the effect was not a one-off finding.
However, we should be careful not to overstate the data. The pivotal acute trials were short, mostly 5 weeks. They tell us that xanomeline–trospium can reduce acute schizophrenia symptoms. They do not yet fully answer long-term questions such as relapse prevention, metabolic outcomes over years, comparative effectiveness against standard antipsychotics, use in treatment-resistant schizophrenia, or real-world tolerability in medically complex patients.
What about cognition?
This is where the story becomes especially interesting.
Cognitive impairment associated with schizophrenia, often called CIAS, is one of the most disabling aspects of the illness. The Cambridge Cognition report notes that patients with schizophrenia often show impairments in processing speed, memory, executive function and social cognition, but also emphasizes that cognition is heterogeneous: some patients perform within the normal range, while others show significant impairment.
A 2025 pooled analysis of two phase 3 trials examined cognition using CANTAB-based composite scores. The analysis prespecified a subgroup of patients who were cognitively impaired at baseline, defined as performing at least 1 standard deviation below norms. In that subgroup, xanomeline–trospium showed significant cognitive improvement compared with placebo, while the authors concluded that this benefit was not attributable simply to improvement in psychotic symptoms.
This is a crucial point: the cognitive signal appears more meaningful when patients are selected or stratified based on actual baseline cognitive impairment. The Cambridge Cognition document similarly emphasizes that including cognitively normal patients in pro-cognitive trials can dilute the ability to detect a true treatment effect.
Why trospium is both useful and clinically important
Trospium is added for a reason, but it also brings monitoring responsibilities. Trospium is an antimuscarinic drug and can cause anticholinergic adverse effects. The prescribing information specifically warns about dry mouth, constipation, dyspepsia, urinary tract infection, urinary retention and central nervous system effects such as dizziness, confusion, hallucinations and somnolence.
This means clinicians must be especially cautious in patients with urinary retention, benign prostatic hyperplasia, narrow-angle glaucoma risk, constipation, gastric retention, renal impairment, hepatic impairment, older age, and polypharmacy. The prescribing information lists contraindications including urinary retention, moderate or severe hepatic impairment, gastric retention, hypersensitivity, and untreated narrow-angle glaucoma.
In clinical practice, the question will not be “Is this a revolutionary drug?” alone. The better question will be: “For which patient, at what stage, with what monitoring, and with what functional target?”
Dosing: not a drug to casually start or copy
The U.S. prescribing information recommends starting at 50 mg/20 mg twice daily, increasing to 100 mg/20 mg twice daily, and then potentially to 125 mg/30 mg twice daily depending on response and tolerability. It should be taken at least 1 hour before food or 2 hours after food, and liver enzymes, bilirubin and heart rate should be assessed before and during treatment as clinically indicated.
This is not a casual “new-generation antipsychotic” to be used without structured assessment. Its place will be best defined through careful diagnosis, symptom profiling, cognitive assessment, medical screening, and longitudinal follow-up.
A balanced clinical interpretation
Xanomeline–trospium is exciting because it opens a non-D2 route in schizophrenia pharmacotherapy. It may be particularly relevant for patients where dopamine blockade produces unacceptable adverse effects, where cognitive and negative symptoms are prominent, or where clinicians want a mechanistically different option.
But it is not a magic bullet. It does not replace comprehensive care. Schizophrenia treatment still requires psychoeducation, family work, relapse prevention, sleep stabilization, substance use assessment, metabolic monitoring, cognitive rehabilitation, vocational support, and careful risk assessment.
The real promise of xanomeline–trospium is not merely that it is a new tablet. Its promise is that it forces psychiatry to think more precisely: Which symptom domain are we treating? Which brain circuit are we targeting? Which cognitive profile does the patient have? Are we measuring recovery only by symptom reduction, or by real-world functioning?
Conclusion
Xanomeline–trospium may mark the beginning of a new chapter in schizophrenia treatment. Its muscarinic mechanism, dopamine-sparing profile, encouraging acute efficacy data and emerging cognition findings make it one of the most important recent developments in psychopharmacology.
The next step is not blind enthusiasm, but intelligent integration: careful patient selection, objective cognitive assessment, safety monitoring, and a recovery-oriented treatment plan.
For psychiatry, this drug is a reminder that schizophrenia is not just a dopamine disorder. It is a disorder of brain networks, cognition, motivation, perception, prediction, salience and social functioning. Treatment must evolve in the same direction.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808