Psychiatrist’s Role in Parkinson’s Disease: Beyond Tremor and Movement
 Parkinson’s disease is commonly understood as a neurological movement disorder causing tremor, slowness, stiffness, reduced facial expression, shuffling gait and imbalance. But for many patients and families, the most difficult part of Parkinson’s disease is not only the movement problem. It is the change in mood, sleep, motivation, thinking, behaviour, personality, confidence, relationships and caregiver burden.
Parkinson’s disease is commonly understood as a neurological movement disorder causing tremor, slowness, stiffness, reduced facial expression, shuffling gait and imbalance. But for many patients and families, the most difficult part of Parkinson’s disease is not only the movement problem. It is the change in mood, sleep, motivation, thinking, behaviour, personality, confidence, relationships and caregiver burden.
This is where the psychiatrist has an important and often under-recognised role.
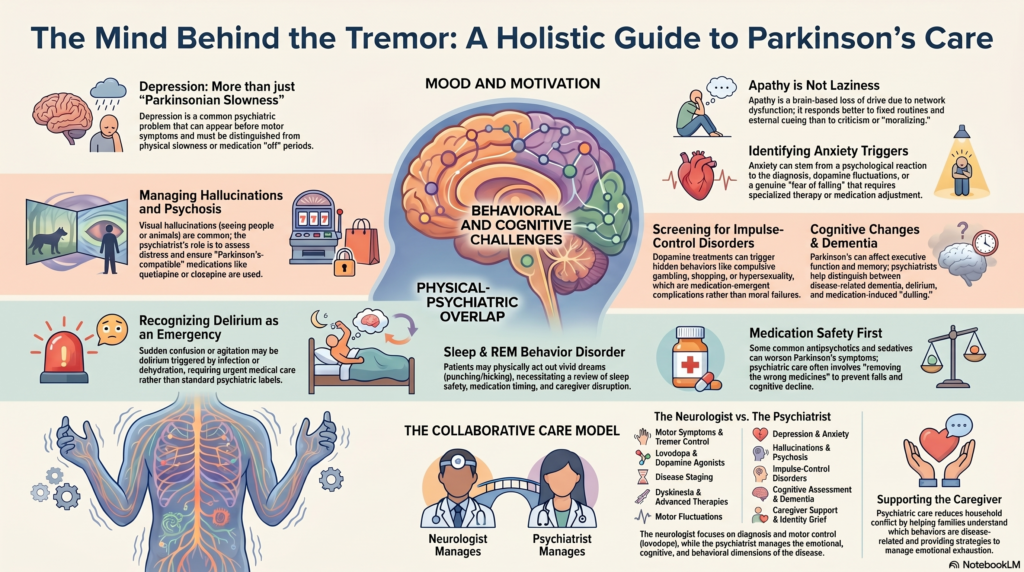
A psychiatrist does not replace the neurologist in Parkinson’s disease. The neurologist remains central for diagnosis, motor symptom control, dopaminergic medicines, disease staging and advanced therapies. The psychiatrist works alongside the neurologist to manage the neuropsychiatric and behavioural dimensions of Parkinson’s disease.
In simple terms, the psychiatrist asks:
What is happening to the person behind the tremor?
Parkinson’s disease is not only a movement disorder
Parkinson’s disease affects several brain systems, including dopaminergic, serotonergic, noradrenergic and cholinergic networks. Because these systems are involved in mood, reward, sleep, attention and cognition, Parkinson’s disease can produce a wide range of non-motor symptoms.
These may include:
depression, anxiety, apathy, sleep disturbance, hallucinations, delusions, impulse-control problems, cognitive decline, Parkinson’s disease dementia, fatigue, irritability, emotional lability, sexual behavioural changes and caregiver distress.
The Parkinson’s Foundation notes that non-movement symptoms can affect mood, thinking and daily wellbeing, and may include depression, anxiety, apathy, cognitive changes, sleep disturbance, fatigue, constipation, bladder issues and pain.
This is why Parkinson’s disease care must go beyond levodopa timing and tremor control. It must include the patient’s emotional and cognitive life.
1. Treating depression in Parkinson’s disease
Depression is one of the most common psychiatric problems in Parkinson’s disease. It may occur before motor symptoms, after diagnosis, during disease progression, or during medication “off” periods.
Depression in Parkinson’s disease may appear as:
low mood, loss of interest, reduced motivation, social withdrawal, fatigue, sleep disturbance, crying spells, irritability, pessimism, hopelessness or reduced confidence.
The challenge is that depression can be difficult to distinguish from Parkinsonian slowness. A patient who speaks softly, moves slowly and sits quietly may be assumed to be “just Parkinsonian,” when they may actually be depressed.
A psychiatrist helps differentiate:
depression from motor slowing,
apathy from sadness,
fatigue from depressive anergia,
medication wearing-off from mood disorder,
adjustment distress from major depressive disorder.
Treatment may include psychoeducation, supportive psychotherapy, behavioural activation, exercise planning, caregiver counselling and antidepressants when clinically indicated. NICE recommends that depression in Parkinson’s disease be identified and managed using guidance for depression in adults with chronic physical illness.
2. Managing anxiety, panic and fear of falling
Anxiety is very common in Parkinson’s disease. Some patients experience persistent worry about disease progression, while others develop panic-like episodes, fear of falling, social embarrassment due to tremor, or anxiety during medication wearing-off states.
Anxiety may present as:
restlessness, inner tension, palpitations, breathlessness, trembling, fear of freezing, fear of public places, sleep difficulty, repeated reassurance-seeking or avoidance of social situations.
A psychiatrist assesses whether anxiety is due to:
psychological reaction to diagnosis,
dopamine fluctuations,
motor “off” periods,
fear of falls,
autonomic symptoms,
depression,
sleep disturbance,
or medication side effects.
This distinction is important because the treatment differs. Some patients need psychotherapy and graded confidence-building. Some need antidepressant treatment. Some need neurologist-led adjustment of Parkinson’s medication if anxiety is tightly linked to wearing-off periods.
3. Understanding apathy: not laziness, but brain-based loss of drive
Apathy is one of the most misunderstood symptoms in Parkinson’s disease.
Families may say:
“He is not trying.”
“She has become lazy.”
“He has lost interest in everything.”
“She just sits silently.”
But apathy is not laziness. It is a reduction in motivation, initiation and emotional drive due to brain network dysfunction. Apathy may occur with depression, but it can also occur without sadness.
A psychiatrist helps families understand that scolding, criticism or repeated moralising rarely helps. Apathy responds better to structure.
Useful approaches include:
fixed daily routines,
external cueing,
pleasant activity scheduling,
small achievable goals,
exercise,
social stimulation,
reducing overstimulation,
reviewing sedating medicines,
and treating co-existing depression or sleep problems.
This reframing is often a turning point for families. The patient is not being deliberately difficult. The brain’s motivation system is affected.
4. Managing hallucinations and Parkinson’s disease psychosis
Psychosis in Parkinson’s disease may include visual hallucinations, illusions, sense of presence, paranoid ideas, suspiciousness or fixed false beliefs. A patient may see people, animals, insects or shadows, especially in dim light or at night.
The psychiatrist’s first role is not to immediately prescribe an antipsychotic. The first role is to assess:
Are the hallucinations distressing?
Does the patient retain insight?
Is there danger to self or others?
Is there delirium?
Is there dementia?
Are medications contributing?
Is sleep deprivation worsening symptoms?
Is there infection, dehydration, pain or metabolic disturbance?
NICE advises that hallucinations and delusions in Parkinson’s disease should not be treated if they are well tolerated by the person, family and carers. When treatment is needed, NICE recommends careful use of Parkinson’s-compatible options: quetiapine may be considered in those without cognitive impairment, clozapine may be offered when standard treatment is not effective, olanzapine should not be offered, and antipsychotics such as phenothiazines and butyrophenones can worsen motor symptoms.
This is a crucial psychiatric safety point. Many commonly used antipsychotics can worsen Parkinsonism, increase falls, cause sedation, worsen swallowing, or impair cognition.
In settings where available, pimavanserin is another important option for Parkinson’s disease psychosis. A recent evidence-based review notes pimavanserin as a first-line choice for mild symptoms, quetiapine when faster improvement is required, and clozapine for urgent or difficult cases.
5. Screening for impulse-control disorders
This is one of the most important psychiatric roles in Parkinson’s disease.
Dopamine agonists and other dopaminergic treatments can sometimes produce impulse-control disorders. These may be hidden due to shame, embarrassment or family conflict.
Symptoms may include:
pathological gambling,
compulsive shopping,
hypersexuality,
binge eating,
excessive internet use,
compulsive hobbyism,
punding,
repetitive purposeless activity,
or compulsive overuse of Parkinson’s medication.
Families may notice sudden financial losses, secretive phone use, excessive spending, sexual disinhibition, irritability when restricted, or repetitive mechanical behaviours.
The psychiatrist helps by:
asking sensitively,
reducing shame,
assessing risk,
involving the family,
managing relationship damage,
treating co-existing depression or anxiety,
and coordinating medication adjustment with the neurologist.
This is not simply a “bad habit” or moral failure. It can be a treatment-emergent neuropsychiatric complication involving dopamine and reward pathways.
6. Assessing cognition and Parkinson’s disease dementia
Parkinson’s disease can affect cognition. The pattern may involve attention, executive function, processing speed, visuospatial ability, memory retrieval and judgement.
A psychiatrist may be consulted when the family notices:
forgetfulness, confusion, hallucinations, poor decision-making, difficulty handling money, medication mistakes, getting lost, unsafe driving, reduced planning ability, or loss of independence.
The psychiatrist helps distinguish:
Parkinson’s disease mild cognitive impairment,
Parkinson’s disease dementia,
delirium,
depression-related cognitive impairment,
Lewy body dementia overlap,
medication-induced cognitive dulling.
NICE recommends cholinesterase inhibitors for mild or moderate Parkinson’s disease dementia, consideration of cholinesterase inhibitors even in severe Parkinson’s disease dementia, and memantine when cholinesterase inhibitors are not tolerated or are contraindicated.
The psychiatrist also helps families plan supervision, safety, financial protection, driving decisions, caregiver support and long-term care.
7. Managing sleep problems and REM sleep behaviour disorder
Sleep disturbance is common in Parkinson’s disease. Patients may have insomnia, fragmented sleep, vivid dreams, daytime sleepiness, restless legs, nocturia, pain, anxiety, night-time confusion or REM sleep behaviour disorder.
REM sleep behaviour disorder is especially important. Patients may shout, kick, punch, fall from bed or act out dreams, sometimes injuring themselves or their spouse.
A psychiatrist assesses:
sleep timing,
dream enactment,
night-time hallucinations,
medication timing,
daytime sleepiness,
co-existing depression or anxiety,
caregiver sleep disruption,
and risk of injury.
Sleep management may involve behavioural strategies, bedroom safety measures, medication review, treatment of anxiety or depression, and coordination with neurology or sleep medicine.
8. Identifying delirium and acute confusion
A Parkinson’s patient who suddenly becomes confused, agitated, suspicious or hallucinating should not automatically be labelled as having “psychiatric worsening.”
Sudden change may indicate delirium.
Common triggers include:
urinary infection, pneumonia, constipation, dehydration, electrolyte imbalance, pain, medication toxicity, poor sleep, hospitalisation or surgery.
This is a medical emergency. The psychiatrist’s role is to recognise delirium early, avoid inappropriate sedatives, review medication risks, and coordinate urgent medical care.
This is particularly important because many usual medications for agitation can worsen Parkinson’s symptoms.
9. Medication safety and avoiding harm
Psychiatric prescribing in Parkinson’s disease needs special caution. Some medicines can worsen stiffness, slowness, cognition, constipation, urinary symptoms, sedation, falls or swallowing difficulty.
A psychiatrist reviews:
anticholinergic burden,
sedating medicines,
benzodiazepine overuse,
dopamine-blocking antipsychotics,
sleep medicines,
pain medicines,
and drug interactions.
This is especially important in older adults who may already be taking multiple medicines for diabetes, hypertension, cardiac disease, sleep, pain or urinary symptoms.
Good psychiatric care in Parkinson’s disease is not just about adding medicines. It is often about removing the wrong medicines.
10. Supporting caregivers and families
Parkinson’s disease affects the entire family.
Caregivers may struggle with:
medication schedules, falls, sleep disruption, hallucinations, sexual behavioural changes, dependence, financial stress, emotional exhaustion, guilt, anger and fear of the future.
A psychiatrist helps the caregiver understand:
what is disease-related,
what is medication-related,
what is psychological,
what is behavioural,
and what can be modified.
Caregiver counselling can reduce conflict. For example, if a spouse understands that apathy is not laziness, hallucinations are not wilful lying, and impulse-control symptoms may be medication-related, the emotional tone of the household changes.
The goal is to protect both the patient and the caregiver.
11. Helping with adjustment, identity and dignity
Parkinson’s disease often affects a person’s identity.
A teacher may feel embarrassed by soft speech.
A professional may avoid meetings due to tremor.
A homemaker may feel distressed by dependence.
A spouse may feel guilty about becoming a burden.
A younger patient may worry about career, marriage, sexuality and finances.
The psychiatrist helps the patient process grief, role change, fear of progression, shame, anger, social withdrawal and loss of autonomy.
This is not merely “counselling.” It is part of preserving personhood.
A patient is not only a set of motor symptoms. They are a person with memories, relationships, responsibilities, pride, fears and hopes.
12. Working closely with the neurologist
The ideal model is collaborative care.
The neurologist manages:
diagnosis, motor symptoms, levodopa and dopamine agonist therapy, motor fluctuations, dyskinesia, advanced therapies, deep brain stimulation and disease progression.
The psychiatrist manages:
depression, anxiety, apathy, psychosis, impulse-control disorders, sleep problems, cognition, delirium, caregiver distress, medication safety and behavioural complications.
Together, the psychiatrist and neurologist can decide whether a symptom is due to:
Parkinson’s disease itself,
dopaminergic medication,
wearing-off phenomena,
depression or anxiety,
sleep disorder,
delirium,
dementia,
or family/environmental stress.
This is the kind of integrated care that Parkinson’s disease patients deserve.
When should a Parkinson’s patient see a psychiatrist?
A psychiatric consultation is useful if the patient has:
persistent sadness or crying spells,
excessive worry or panic,
loss of interest and motivation,
sleep disturbance,
visual hallucinations,
suspiciousness,
confusion,
memory decline,
anger or irritability,
sexual disinhibition,
compulsive spending or gambling,
binge eating,
caregiver conflict,
suicidal thoughts,
or difficulty adjusting to the diagnosis.
Families should not wait until symptoms become severe. Early psychiatric involvement can prevent crises, reduce caregiver burden and improve quality of life.
Conclusion
The psychiatrist’s role in Parkinson’s disease is not peripheral. It is central to whole-person care.
A neurologist may improve movement, but the psychiatrist helps preserve the patient’s emotional life, cognitive functioning, behavioural stability, family relationships and dignity.
For families, this means one important message:
If a person with Parkinson’s disease develops depression, anxiety, hallucinations, memory problems, sleep disturbance, behavioural change or caregiver distress, psychiatric care can make a meaningful difference.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808