Narcolepsy: Understanding the Sleep Disorder That Blurs the Boundary Between Wakefulness and Dreaming
 Narcolepsy is often misunderstood as “just excessive sleepiness.” In reality, it is a chronic neurological disorder in which the brain struggles to regulate the sleep–wake cycle properly. A person with narcolepsy may wake up feeling reasonably refreshed, yet experience overwhelming sleepiness during the day. They may fall asleep suddenly, struggle to stay alert during work or study, and experience unusual phenomena such as sleep paralysis, vivid hallucinations, or sudden weakness triggered by emotions.
Narcolepsy is often misunderstood as “just excessive sleepiness.” In reality, it is a chronic neurological disorder in which the brain struggles to regulate the sleep–wake cycle properly. A person with narcolepsy may wake up feeling reasonably refreshed, yet experience overwhelming sleepiness during the day. They may fall asleep suddenly, struggle to stay alert during work or study, and experience unusual phenomena such as sleep paralysis, vivid hallucinations, or sudden weakness triggered by emotions.
Narcolepsy can significantly affect academic performance, occupational functioning, emotional wellbeing, driving safety, relationships, and self-esteem. Because symptoms are often mistaken for laziness, depression, seizure disorder, poor motivation, or behavioural problems, many people remain undiagnosed for years.
How Normal Sleep Works
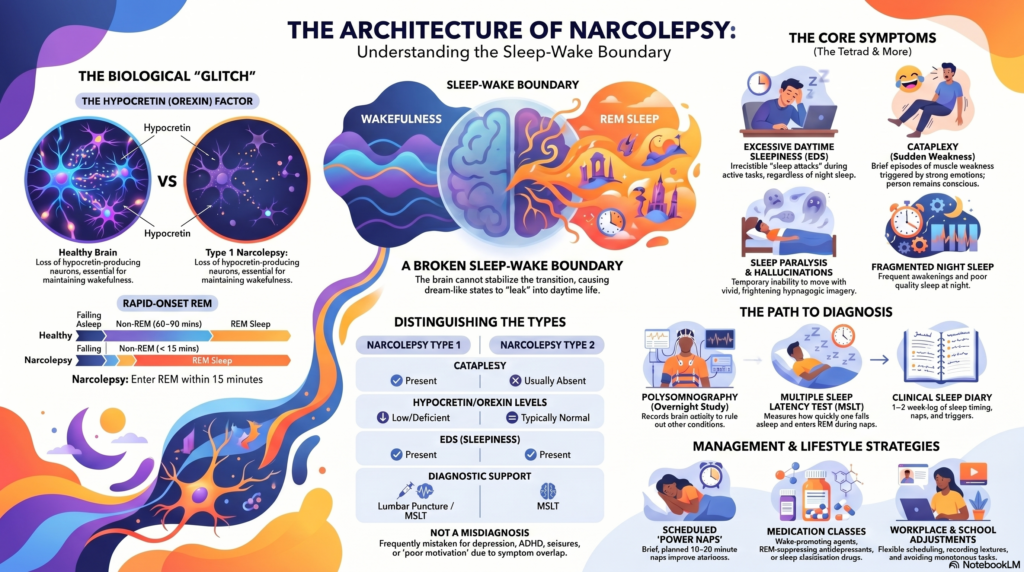
A typical sleep cycle moves through non-REM sleep stages before entering REM sleep after about 60–90 minutes. REM sleep is the stage in which dreaming is most prominent. During REM sleep, the brain temporarily reduces muscle tone so that we do not physically act out our dreams.
In narcolepsy, this boundary between wakefulness, non-REM sleep, and REM sleep becomes unstable. REM-related phenomena may intrude into wakefulness. This explains why people with narcolepsy may enter REM sleep very quickly, sometimes within 15 minutes of falling asleep. It also explains symptoms such as sleep paralysis, dream-like hallucinations, and cataplexy.
Core Symptoms of Narcolepsy
1. Excessive Daytime Sleepiness
Excessive daytime sleepiness is the most universal symptom. The person may feel an irresistible urge to sleep, sometimes described as a “sleep attack.” These episodes can occur during classes, meetings, conversations, travel, or even while eating.
Importantly, this sleepiness is not simply due to poor discipline or inadequate motivation. Even after adequate nighttime sleep, the person may continue to feel sleepy during the day.
2. Cataplexy
Cataplexy refers to sudden episodes of muscle weakness triggered by strong emotions such as laughter, anger, surprise, excitement, fear, or stress. It may be subtle, such as drooping eyelids, head nodding, slurred speech, jaw weakness, or buckling of the knees. In severe cases, the person may collapse completely.
A key point is that consciousness is preserved. The person remains aware but may be unable to move or speak for a few seconds to a few minutes. This helps differentiate cataplexy from fainting or epileptic seizures.
3. Sleep Paralysis
Sleep paralysis is the temporary inability to move or speak while falling asleep or waking up. It may last a few seconds or minutes but can be extremely frightening. The person may feel awake but unable to move, sometimes with a sense of pressure, fear, or presence in the room.
4. Hypnagogic and Hypnopompic Hallucinations
These are vivid dream-like experiences occurring while falling asleep or waking up. They may be visual, auditory, or tactile. A person may hear voices, see figures, feel touched, or experience frightening dream-like imagery. These are not necessarily psychotic symptoms; they can be part of REM sleep intruding into wakefulness.
5. Fragmented Night Sleep
Paradoxically, people with narcolepsy are sleepy during the day but may sleep poorly at night. They may wake repeatedly, experience vivid dreams, insomnia, sleep apnea, leg movements, or dream enactment behaviours.
6. REM Sleep Behaviour Disorder-like Symptoms
Usually, during REM sleep, muscles are temporarily paralysed. In REM sleep behaviour disorder, this paralysis is reduced or absent, causing the person to act out dreams by shouting, punching, kicking, or moving during sleep. This can disturb the person and their bed partner and may sometimes coexist with narcolepsy.
Types of Narcolepsy
Narcolepsy Type 1
Narcolepsy Type 1 is associated with cataplexy and low levels of hypocretin, also called orexin. Hypocretin is a brain chemical that helps maintain wakefulness and stabilise REM sleep regulation.
A person may be diagnosed with Type 1 narcolepsy if they have excessive daytime sleepiness, cataplexy, and supportive findings on sleep testing, or if hypocretin levels are found to be low.
Narcolepsy Type 2
Narcolepsy Type 2 presents with excessive daytime sleepiness but usually without cataplexy. Hypocretin levels are typically normal or less clearly reduced. Symptoms may be milder, but they can still significantly impair daily life.
Secondary Narcolepsy
Rarely, narcolepsy may occur due to injury, tumour, inflammation, or disease affecting the hypothalamus, the brain region involved in sleep–wake regulation. In such cases, other neurological symptoms may also be present.
Why Does Narcolepsy Happen?
The exact cause is not fully understood, but Type 1 narcolepsy is strongly linked to loss of hypocretin-producing neurons in the hypothalamus. Current research suggests that this may occur through an autoimmune process in genetically susceptible individuals.
One genetic association is with HLA-DQB1*06:02. This does not mean that everyone with this gene will develop narcolepsy, but it increases susceptibility. Environmental triggers such as infections may activate immune mechanisms in vulnerable individuals. Some research has linked narcolepsy onset with infections such as streptococcal illness or influenza-like illnesses.
In short, narcolepsy is not a psychological weakness. It is a brain-based sleep–wake regulation disorder.
Why Narcolepsy Is Often Missed
Narcolepsy can be mistaken for several other conditions, including:
Depression, ADHD, seizure disorder, chronic fatigue, laziness, poor motivation, dissociation, anxiety, substance use, medication sedation, or behavioural problems.
In children and adolescents, narcolepsy may present as poor academic performance, irritability, emotional outbursts, inattentiveness, weight gain, social withdrawal, or sudden falls. Because of this, a careful sleep history is essential.
Diagnosis of Narcolepsy
Diagnosis requires a detailed clinical evaluation and usually specialised sleep testing.
1. Clinical History
The doctor will ask about daytime sleepiness, sleep attacks, cataplexy, sleep paralysis, hallucinations, nighttime sleep quality, snoring, medications, psychiatric symptoms, neurological symptoms, and family history.
A sleep diary for one to two weeks can be useful. It helps document sleep timing, naps, sleep attacks, nighttime awakenings, and triggers.
2. Polysomnography
Polysomnography, or overnight sleep study, records brain activity, eye movements, muscle activity, breathing, oxygen levels, and body movements during sleep. It helps rule out other conditions such as obstructive sleep apnea, periodic limb movement disorder, parasomnias, and insufficient sleep.
3. Multiple Sleep Latency Test
The Multiple Sleep Latency Test, or MSLT, is performed during the day after an overnight sleep study. The person is given several nap opportunities. The test measures how quickly they fall asleep and whether they enter REM sleep unusually early.
Short sleep latency and sleep-onset REM periods support the diagnosis of narcolepsy.
4. Hypocretin Testing
In selected cases, hypocretin-1 levels may be measured in cerebrospinal fluid through lumbar puncture. Very low levels strongly support Narcolepsy Type 1.
Treatment of Narcolepsy
Narcolepsy is usually a lifelong condition, but symptoms can be managed. Treatment is individualised and often combines medication, behavioural strategies, safety planning, psychoeducation, and support.
Medication Options
Wake-Promoting Agents
Modafinil, armodafinil, and solriamfetol are commonly used to reduce excessive daytime sleepiness. They help improve alertness and functioning during the day.
Stimulants
Methylphenidate or amphetamine-like stimulants may be used when sleepiness is severe or not adequately controlled with wake-promoting agents. These require careful monitoring because of possible cardiovascular, appetite, sleep, and misuse-related concerns.
Medicines for Cataplexy
Cataplexy may respond to certain antidepressants, especially drugs that suppress REM sleep. These include venlafaxine, fluoxetine, clomipramine, imipramine, and other related agents. The choice depends on the person’s symptom profile, comorbidities, and tolerability.
Sodium Oxybate and Low-Sodium Oxybate
These medicines can improve cataplexy and excessive daytime sleepiness in selected patients. Because of safety issues and misuse potential, their availability and regulation vary across countries.
Pitolisant
Pitolisant acts through the histamine system and can help with excessive daytime sleepiness and cataplexy. It is a non-stimulant wake-promoting medication in some regulatory settings.
Lifestyle and Behavioural Strategies
Medication alone is often not enough. Behavioural planning can make a major difference.
Scheduled Short Naps
Planned naps of 10–20 minutes at strategic times can reduce sleep attacks and improve functioning.
Regular Sleep Schedule
Going to bed and waking up at consistent times helps stabilise the sleep–wake rhythm.
Avoid Alcohol and Late Caffeine
Alcohol fragments sleep and may worsen sleep quality. Caffeine late in the day can worsen nighttime insomnia.
Exercise
Regular exercise, preferably earlier in the day, can improve sleep quality, mood, and daytime alertness.
Light Evening Meals
Heavy meals late at night can worsen sleep quality. Some individuals also feel more sleepy after carbohydrate-heavy meals.
Safety Planning
People with narcolepsy should avoid driving when sleepy. Driving, operating machinery, swimming alone, working at heights, and cooking with fire may require precautions depending on symptom severity.
Psychological Impact of Narcolepsy
Narcolepsy can affect more than sleep. Many patients experience shame, frustration, low self-confidence, anxiety, depression, or social embarrassment. Repeated criticism from others — “lazy,” “careless,” “not serious” — can damage self-worth.
This is especially important in adolescents and young adults. A person who has spent years being misunderstood may internalise blame. Psychoeducation, supportive therapy, CBT-based strategies, and family counselling can help restore confidence and improve adaptation.
Narcolepsy and School or Workplace Adjustments
People with narcolepsy may benefit from reasonable accommodations such as:
Flexible scheduling, planned nap breaks, avoiding long monotonous tasks, permission to record lectures, sitting in alertness-promoting environments, task planning during peak alert periods, and reduced stigma through awareness.
Children and adolescents may need coordination between doctors, parents, and schools. Adults may require workplace planning, especially if their job involves driving, machinery, long meetings, or shift work.
Future Directions: Orexin-Based Therapies
A major area of research is orexin-based treatment. Since Type 1 narcolepsy is linked to hypocretin/orexin deficiency, future therapies may aim to replace orexin, stimulate orexin receptors, or restore orexin-related signalling. These treatments may eventually target the underlying mechanism more directly rather than only managing symptoms.
Key Takeaway
Narcolepsy is a neurological sleep disorder, not laziness, weakness, or lack of discipline. It occurs when the brain cannot properly stabilise wakefulness and REM sleep. The result can be excessive daytime sleepiness, cataplexy, sleep paralysis, vivid hallucinations, fragmented sleep, and major functional impairment.
With proper diagnosis, sleep testing, medication, lifestyle planning, safety precautions, and psychological support, people with narcolepsy can study, work, maintain relationships, and live meaningful lives.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Chennai
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Narcolepsy Beyond the Pentad: Why “CHESS” Is Only the Opening Move
- Exploring Alternatives to Methylphenidate: A Guide for ADHD and Narcolepsy Management in India
- The Complex Relationship Between Trauma and Adult Sexuality: Understanding the Impact and Path to Healing
- AuDHD: Understanding the Overlap Between Autism and ADHD
- The Alarming Link Between Alcohol and Six Major Cancers: What You Need to Know
- How ADHD Stimulant Medications Really Work: Dopamine, Transporters, and the Fine Line Between Therapy and Toxicity