What Really Happens During a Psychiatry Consultation?
 A Clear, Reassuring Guide for Anyone Visiting a Psychiatrist for the First Time
A Clear, Reassuring Guide for Anyone Visiting a Psychiatrist for the First Time
For many people, the hardest part of psychiatric treatment is not taking medication or discussing painful experiences.
It is booking the first appointment.
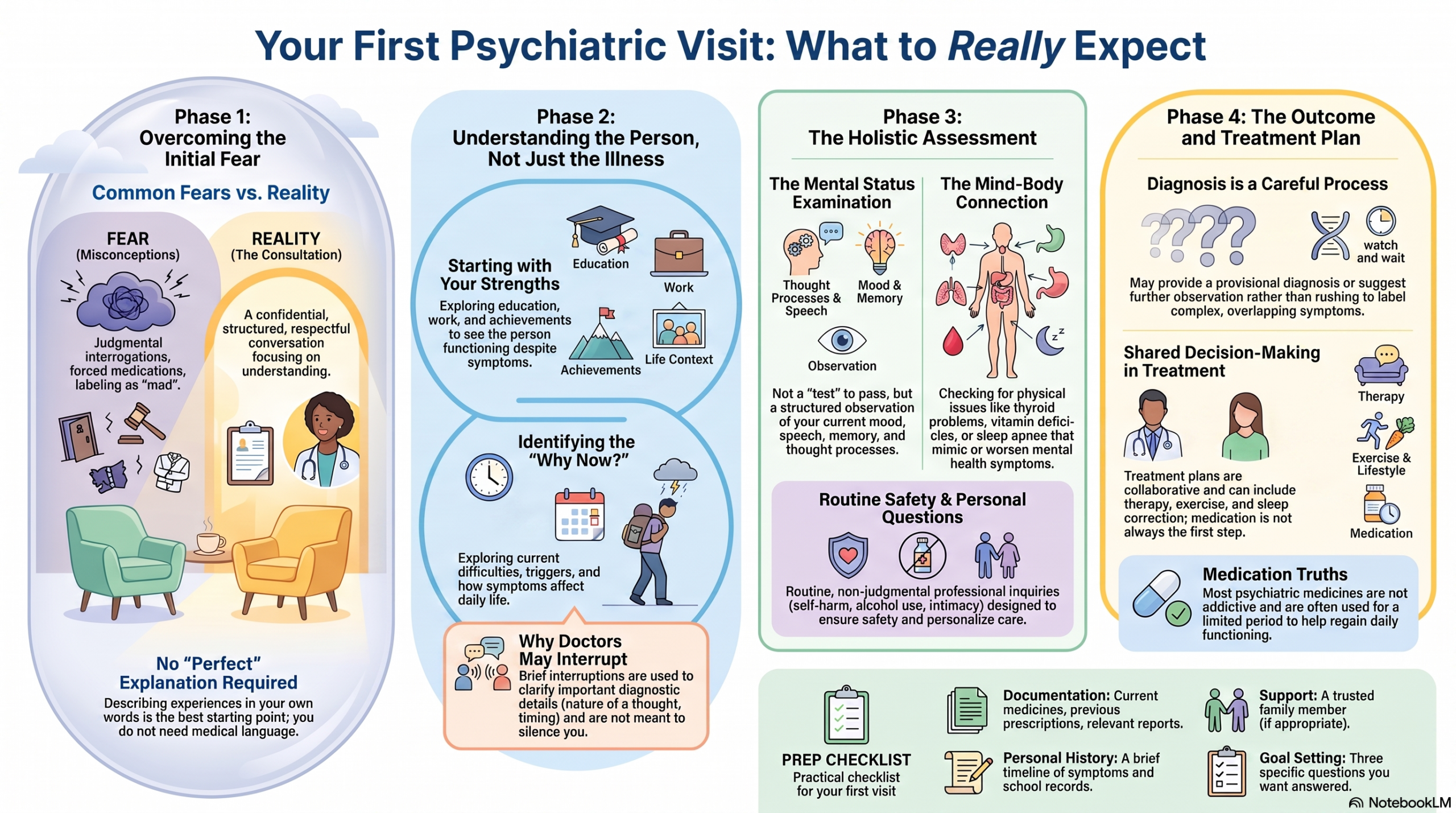
Before meeting a psychiatrist, people often carry many fears:
“Will the doctor think I am mad?”
“Will I be forced to take tablets?”
“What if I cry?”
“What if I cannot explain my problem properly?”
“Will my family be told everything?”
“What if my problem is too small for a psychiatrist?”
These concerns are understandable. Psychiatric consultations are rarely shown realistically in films or television. People may imagine an interrogation, a judgemental doctor, or an immediate diagnosis based on a few questions.
A proper psychiatric consultation is very different.
It is a confidential, structured and respectful conversation designed to understand what you are experiencing, why it may be happening, how it is affecting your life and what can be done to help.
You do not need to prepare a perfect explanation. You do not need to know the name of your condition. You do not need to decide in advance whether you want medication or therapy.
You only need to begin the conversation.
I usually begin by understanding the person—not the illness
I do not like to begin a consultation with:
“What is wrong with you?”
A person who comes to a psychiatric clinic may already have spent months thinking about everything that is wrong.
They may have been described as lazy, weak, stubborn, short-tempered, overdramatic, careless, irresponsible or difficult.
They may already feel that their symptoms have replaced their identity.
So I often begin differently.
I may ask:
“Tell me a few good things about yourself.”
“What did you study?”
“What kind of work do you do?”
“What are you good at?”
“What have you managed well in your life?”
“What do your friends or family appreciate about you?”
Some people are surprised by these questions. A few struggle to answer because they have become so focused on their difficulties that they have forgotten their strengths.
But these questions are not casual conversation.
Your education, work, interests, achievements, responsibilities and relationships tell me something important about the person behind the symptoms.
Before discussing depression, I want to know the person who has been functioning despite depression.
Before discussing ADHD, I want to understand the creativity, intelligence and effort that may have helped someone compensate for years.
Before discussing anxiety, I want to know how much the person has continued to do despite fear.
Psychiatry should never reduce a human being to a diagnosis.
Then I ask what brought you to the consultation
After understanding a little about you, the conversation gradually moves towards the present difficulty.
The psychiatrist may ask:
“What made you decide to seek help now?”
“What has been troubling you recently?”
“When did you first notice a change?”
“How is this affecting your day-to-day life?”
There is no correct way to tell your story.
Some people begin with a symptom:
“I am not sleeping.”
Others begin with an event:
“Everything changed after my mother died.”
Some begin with a relationship problem:
“My husband says I have become very irritable.”
Others may say:
“I don’t know what is wrong. I just don’t feel like myself.”
All these are valid starting points.
You do not have to speak in medical language. You do not need to say “I have major depressive disorder” or “I think I have generalised anxiety disorder.”
You can simply describe what you are experiencing in your own words.
The psychiatrist listens to both symptoms and the story around them
A psychiatric symptom cannot be understood properly without context.
For example, saying “I cannot concentrate” is only the beginning.
The psychiatrist may need to understand:
- Whether concentration problems began in childhood or only recently
- Whether they occur at work, at home or everywhere
- Whether they worsen during stress
- Whether sleep is poor
- Whether there is anxiety, depression or substance use
- Whether the person is distracted, mentally slowed or preoccupied
- Whether memory is also affected
- Whether any medicine or physical illness could be contributing
Similarly, “I am not sleeping” can mean several different things.
One person may lie awake worrying for hours.
Another may sleep only three hours but still feel energetic and unusually active.
A third may sleep during the day because of night-shift work.
A fourth may have sleep apnoea.
The same complaint can arise from very different causes. That is why psychiatric interviewing involves careful clarification rather than simply matching one symptom to one diagnosis.
Why psychiatrists sometimes interrupt
People sometimes worry that the doctor is interrupting them because their story is unimportant.
A good psychiatric consultation should give you enough space to speak freely. Your spontaneous account reveals what matters most to you, how you understand the problem and what emotions are attached to it.
However, the psychiatrist may occasionally interrupt to clarify something important.
For example:
“When you say you heard a voice, did it sound as if someone was speaking from outside, or was it more like a thought in your own mind?”
“When you say you did not sleep, were you tired but unable to sleep, or did you not feel the need for sleep?”
“When you say you were scared of contamination, did you believe contamination had definitely occurred, or were you worried that it might have occurred?”
“Did this difficulty begin before or after the stressful event?”
These distinctions can be diagnostically important.
The purpose of interruption should not be to silence you. It should be to organise the story, establish chronology, assess safety and avoid missing important details.
A good consultation moves between two modes: allowing the person to speak freely and asking focused questions when clarification is needed.
We discuss how the problem affects everyday life
Psychiatric treatment is not only about reducing symptoms.
It is about helping you function better.
The psychiatrist may ask how the problem affects:
- Work or studies
- Marriage and relationships
- Parenting
- Sleep and energy
- Appetite and physical health
- Social life
- Financial decisions
- Driving
- Sexual functioning
- Motivation
- Self-care
- Memory and concentration
- Alcohol, tobacco or other substance use
This is important because two people with the same diagnosis may require completely different treatment plans.
A student with anxiety before examinations has different needs from a business owner who cannot make decisions because of depression.
A homemaker experiencing panic attacks while travelling alone has different practical difficulties from a software professional having panic attacks during meetings.
Treatment should fit the person’s actual life.
Your childhood and past may be discussed—but not to blame anyone
People sometimes worry that psychiatry will involve blaming parents for everything.
That is not the purpose.
Childhood experiences may be discussed because they can help explain long-term patterns in attention, emotions, relationships, coping and self-esteem.
The psychiatrist may ask about:
- Early development
- School performance
- Attention and behaviour in childhood
- Friendships
- Family atmosphere
- Significant losses
- Bullying
- Trauma
- Academic difficulties
- Previous emotional or behavioural problems
This is especially relevant when evaluating conditions such as ADHD, autism-spectrum presentations, learning disorders, personality difficulties, trauma-related disorders or long-standing anxiety.
The aim is not to find someone to blame. It is to understand how the person developed and what patterns may still be influencing the present.
Physical health is also part of psychiatric assessment
The mind and body are not separate systems.
Thyroid problems, anaemia, vitamin deficiencies, hormonal changes, sleep disorders, neurological conditions, infections and certain medications can sometimes produce or worsen psychiatric symptoms.
The psychiatrist may ask about:
- Diabetes, blood pressure and thyroid disease
- Seizures, head injury or neurological illness
- Menstrual, pregnancy or menopausal concerns
- Current medicines
- Steroid use
- Pain conditions
- Snoring and sleep quality
- Alcohol or substance use
- Recent laboratory investigations
In selected cases, blood tests, imaging, sleep assessment or referral to another medical specialist may be advised.
Not every person needs extensive investigations. Tests are selected based on the symptoms, age, medical history and clinical findings.
The family history can provide useful clues
The psychiatrist may ask whether close relatives have experienced depression, bipolar disorder, anxiety, addiction, suicide, dementia, psychosis, ADHD or other mental-health conditions.
This does not mean that the same condition is inevitable.
Family history is simply one part of the overall assessment. Mental-health conditions usually arise from a combination of biological vulnerability, developmental experiences, stress, relationships, sleep, physical health and social circumstances.
Family history helps the psychiatrist understand risk and choose treatment more carefully.
Questions about alcohol, substances and sexual health are routine
Some questions may feel personal.
You may be asked about alcohol, tobacco, cannabis, sleeping tablets, pain medicines or other substances. You may also be asked about sexual functioning, relationship intimacy or impulsive behaviour.
These questions are not moral judgements.
Substances can affect sleep, anxiety, mood, memory and the effectiveness of medication. Sexual symptoms can also arise from depression, anxiety, relationship stress, hormonal changes or medicines.
Accurate information allows safer and more personalised treatment.
You do not need to feel embarrassed. Psychiatrists are trained to discuss sensitive subjects professionally.
Safety questions are a normal part of the consultation
A psychiatrist may ask directly:
“Have you felt that life is not worth living?”
“Have you had thoughts of harming yourself?”
“Have you made any plans?”
“Do you feel unsafe at home?”
These questions are not meant to frighten you or suggest that the doctor assumes the worst.
They are routine questions intended to assess safety.
Answering honestly does not automatically mean hospital admission. Thoughts of death can range from brief feelings of hopelessness to immediate danger. The psychiatrist needs to understand the intensity, frequency, intent, planning and available support.
When there is a serious or immediate safety concern, additional support may be required. This could include involving a trusted person, arranging closer follow-up, modifying medication, creating a safety plan or recommending hospital care.
The goal is protection, not punishment.
What is the Mental Status Examination?
During the consultation, the psychiatrist is not only listening to the content of your words. They are also observing how you are feeling and functioning in the present moment.
This is called the mental status examination.
It may include observations about:
- Appearance and self-care
- Eye contact
- Level of activity
- Speech
- Mood and emotional expression
- Thought process
- Unusual beliefs or perceptions
- Attention and concentration
- Memory
- Insight and judgement
This is not a test you need to pass.
You are not expected to behave in a particular way.
The psychiatrist is simply forming a structured understanding of your current mental state, just as another doctor might examine breathing, pulse or reflexes.
Will I be given a diagnosis immediately?
Sometimes the diagnosis is reasonably clear after the first consultation.
At other times, the psychiatrist may need more information.
Psychiatric symptoms often overlap.
Poor concentration may occur in ADHD, anxiety, depression, sleep deprivation, trauma, substance use, bipolar disorder or medical illness.
Mood swings may represent ordinary emotional reactions, personality patterns, trauma-related instability, premenstrual changes or bipolar disorder.
Repetitive thoughts may be worry, rumination, obsession, trauma memories or suspiciousness.
A careful psychiatrist does not rush to label every symptom.
The first consultation may therefore end with:
- A clear diagnosis
- A provisional diagnosis
- A list of possible explanations
- A recommendation for further assessment
- A plan to observe symptoms over time
Diagnostic caution is not uncertainty due to incompetence. In many cases, it reflects good clinical practice.
Are questionnaires or psychological tests required?
Not everyone needs formal testing.
For many people, a detailed clinical interview is sufficient.
In selected cases, the psychiatrist may recommend structured assessments for:
- Depression
- Anxiety
- ADHD
- Autism-spectrum features
- Obsessive-compulsive symptoms
- Personality functioning
- Memory and cognition
- Learning difficulties
- Attention and executive functioning
- Neuropsychological performance
These tests should support the clinical interview, not replace it.
A questionnaire cannot fully understand your relationships, life history, coping style or the meaning of your symptoms. It provides one additional source of information.
Will the psychiatrist force me to take medication?
No good psychiatric consultation should begin with the assumption that every person needs medication.
Treatment depends on the diagnosis, severity, duration, risk, level of impairment, personal preference and previous response.
For some people, education, sleep correction, exercise, stress management and therapy may be sufficient.
For others, medication may significantly reduce symptoms and help them regain functioning.
In many cases, the most effective approach is a combination of medication, psychological therapy and lifestyle changes.
When medication is advised, the psychiatrist should explain:
- Why it is being recommended
- What improvement is expected
- How long it may take to work
- Common side effects
- Important precautions
- How long it may be required
- What follow-up is needed
- What alternatives are available
You should have the opportunity to ask questions.
Shared decision-making does not mean that the doctor merely agrees with every request. It means that medical recommendations are explained clearly and the patient’s concerns and preferences are taken seriously.
Psychiatric medicines are not all addictive
A common fear in Chennai and elsewhere is:
“Once I start psychiatric tablets, I will have to take them for life.”
This is not true for most people.
Some psychiatric medicines are used for a limited period. Others may be continued longer when there is a high risk of relapse or when the condition is recurrent.
Certain sedative medicines can cause dependence if used inappropriately or for extended periods, which is why they must be prescribed and reviewed carefully. However, antidepressants, mood stabilisers, antipsychotic medications and ADHD treatments cannot all be placed into one category.
The duration of treatment depends on the illness, number of previous episodes, severity, response and individual risk.
Medicines should not be stopped suddenly without medical guidance. When discontinuation is appropriate, it is usually planned gradually.
Therapy is not simply “talking about problems”
Psychological therapy is a structured form of treatment.
Depending on the difficulty, therapy may help a person:
- Recognise unhelpful thinking patterns
- Manage anxiety and panic
- Reduce compulsions
- Improve emotional regulation
- Process trauma
- Develop relationship skills
- Improve organisation and procrastination
- Cope with grief
- Change addictive behaviours
- Understand long-standing personality patterns
The psychiatrist may provide psychotherapy, recommend a clinical psychologist, or combine medical and psychological treatment.
Not every patient requires the same type of therapy. The method should match the problem and the person’s needs.
What happens if a family member comes with me?
Family members can provide useful information, especially when there are concerns about memory, mania, psychosis, addiction, severe depression or childhood-onset symptoms.
However, the patient remains the centre of the consultation.
Whenever possible, part of the discussion may be conducted with the patient alone. This allows the person to speak freely about sensitive concerns.
Family involvement should support treatment, not take control away from the patient.
In some situations, the patient’s account and the family’s account may differ. This does not automatically mean that one person is lying. Different people may notice different parts of the problem.
The psychiatrist’s role is to understand both perspectives fairly.
Is the consultation confidential?
Psychiatric consultations are treated with professional confidentiality.
What you share is not casually discussed with relatives, employers or other people.
However, confidentiality is not completely without limits. When there is an immediate and serious risk to the patient or another person, or when disclosure is required in specific professional circumstances, the psychiatrist may need to take steps to protect safety.
When appropriate, this should be explained clearly.
Fear of judgement or exposure should not prevent you from seeking help. Sensitive issues are a routine part of psychiatric practice.
What if I cry or cannot speak properly?
Crying during a psychiatric consultation is not a failure.
You do not need to apologise.
Some people cry because they are remembering something painful. Others cry because they finally feel permitted to speak. Some become silent because they do not know where to begin.
All of this is acceptable.
You can pause.
You can ask for water.
You can say, “I am finding this difficult to talk about.”
You can write down important points before the appointment or show the psychiatrist a note on your phone.
The consultation does not have to be perfect to be useful.
What should you bring to the first appointment?
You can attend without elaborate preparation. However, it may be useful to bring:
- A list of current medicines
- Previous psychiatric prescriptions
- Relevant medical reports
- Details of previous treatment responses
- A brief timeline of important symptoms
- School records or childhood information when ADHD or learning difficulties are being evaluated
- A family member who knows the history well, when appropriate
It can also help to note three questions you want answered. People sometimes forget important concerns once the consultation begins.
What happens at the end of the consultation?
A good psychiatric consultation should not end with a prescription alone.
By the end, you should ideally understand:
- What the psychiatrist thinks may be happening
- Whether the diagnosis is confirmed or provisional
- What treatment is being recommended
- What improvement to expect
- What side effects or warning signs to watch for
- When follow-up is needed
- What to do if symptoms worsen
- Whether therapy or further assessment is required
The aim is to replace confusion with a workable plan.
Even when the problem cannot be solved immediately, understanding it clearly can itself bring relief.
Many patients say:
“For the first time, what I am experiencing makes sense.”
That is often the beginning of recovery.
Follow-up consultations are different from the first visit
The first consultation is usually about understanding the history and creating a treatment plan.
Follow-up visits focus on:
- Changes in symptoms
- Sleep, appetite and energy
- Work, studies and relationships
- Medication response
- Side effects
- Therapy progress
- New stressors
- Adherence to the plan
- Whether the diagnosis or treatment needs revision
Follow-up is not merely for renewing prescriptions.
It helps the psychiatrist understand whether treatment is improving real-life functioning.
A person may say that their anxiety is “slightly better,” but the more meaningful change may be that they have started driving again, attending meetings, sleeping independently or reconnecting with friends.
These functional improvements matter.
Your problem does not need to be “severe enough”
You do not have to wait until you are unable to work, sleep or care for yourself.
You can consult a psychiatrist for:
- Persistent anxiety
- Repeated panic attacks
- Low mood
- Excessive anger or irritability
- Poor sleep
- Relationship difficulties
- Work-related distress
- ADHD symptoms
- Obsessive thoughts
- Addiction
- Grief
- Memory concerns
- Behavioural changes
- Emotional instability
- Unexplained changes in personality
- Difficulty coping with a major life event
Early treatment is often simpler than waiting until the problem becomes severe.
A psychiatric consultation is not only for people with dramatic or disabling illness. It is also for people who sense that something has changed and want to understand it before it worsens.
The aim is not to change your personality
Many people worry:
“Will treatment make me a different person?”
Appropriate psychiatric treatment should not erase your personality.
The aim is to reduce the symptoms that prevent your personality from being expressed fully.
Depression may make a warm person withdraw.
Anxiety may make a capable person avoid opportunities.
ADHD may prevent an intelligent person from completing what they start.
OCD may consume hours of someone’s day.
Treatment does not remove the person. It helps the person regain freedom from the illness.
A psychiatric consultation should leave you with dignity and hope
The most important outcome of the first consultation is not necessarily a diagnosis or prescription.
It is the feeling that you have been understood.
A good psychiatric consultation should communicate:
“Your difficulty is real.”
“You are not weak.”
“There may be an understandable explanation.”
“You do not have to manage this alone.”
“There is a plan.”
The first appointment is not an examination you need to pass.
It is not an interrogation.
It is not a place where your character is judged.
It is a professional conversation aimed at helping you understand your mind, reduce suffering and return to a more meaningful life.
For someone who has been silently struggling for months or years, that conversation can be the first major step towards recovery.
About the Author
Dr. Srinivas Rajkumar T
MD Psychiatry — AIIMS, New Delhi
Senior Consultant Psychiatrist
Mind & Memory Clinic
Apollo Clinic, Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
At Mind & Memory Clinic, the consultation begins with the person—not merely the symptoms. The aim is to provide careful diagnosis, clear explanations and personalised treatment in a respectful, non-judgemental setting.
You do not need to reach a crisis before seeking help. Sometimes the most important step is simply having an honest conversation.
Related posts:
- Why Psychiatrists Interrupt During a Consultation—and Why It May Be Good Clinical Practice
- What Happens During a Ketamine-Assisted Therapy Session? Step-by-Step Guide for First-Timers
- How to Prepare for Your First Online Psychiatry Consultation
- Step-by-Step Guide: Booking an Online Psychiatry Consultation with Dr. Srinivas
- Online Psychiatry Consultation – Empowering Mental Health Through Virtual Therapy
- 🧠 Consultation–Liaison Psychiatry: Where Medicine Meets the Mind