Sequenced treatment alternatives to relieve depression : A STAR*D-Based, Modern Guideline-Informed Approach
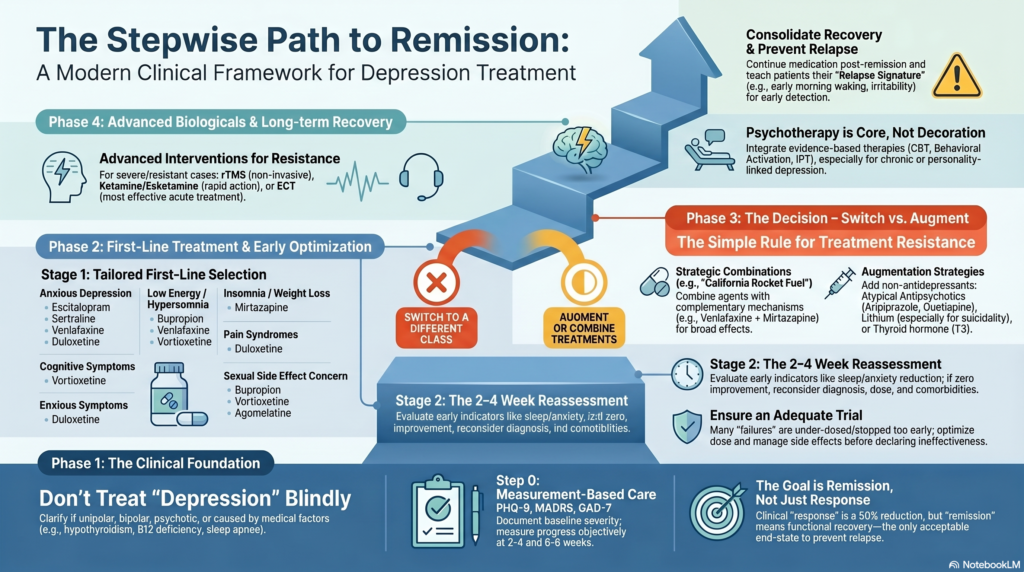 Depression treatment should not be a random trial of one tablet after another. A good psychiatrist approaches depression stepwise: confirm the diagnosis, assess severity and risk, choose the first treatment carefully, measure response, optimise the dose and duration, and then decide whether to switch, combine, augment, use psychotherapy, or move to advanced biological treatments such as rTMS, ketamine/esketamine or ECT.
Depression treatment should not be a random trial of one tablet after another. A good psychiatrist approaches depression stepwise: confirm the diagnosis, assess severity and risk, choose the first treatment carefully, measure response, optimise the dose and duration, and then decide whether to switch, combine, augment, use psychotherapy, or move to advanced biological treatments such as rTMS, ketamine/esketamine or ECT.
The STAR*D trial remains one of the most important real-world studies in depression because it showed what happens when treatment is delivered in sequenced steps. The key lesson was not that one particular antidepressant is magical. The lesson was that depression often needs measurement-based, stepwise, persistent care. About one-third of participants remitted after the first citalopram step, and remission became progressively harder with later steps, with lower acute remission and higher relapse rates when more treatment steps were needed.
Modern guidelines now build on this idea but add newer options: vortioxetine, agomelatine where available, mirtazapine combinations, atypical antipsychotic augmentation, lithium, thyroid hormone, ketamine/esketamine, rTMS, ECT, structured psychotherapy, lifestyle interventions and relapse-prevention planning. CANMAT’s 2023 update provides a contemporary evidence-informed framework for adult major depressive disorder, while NICE NG222 covers first-line and further-line treatment, relapse prevention, chronic depression, psychotic depression and treatment-resistant depression.
First principle: do not treat “depression” blindly
Before choosing medication, the psychiatrist must clarify what kind of depression this is.
A proper assessment asks:
Is this unipolar major depression?
Is there bipolar depression hidden behind it?
Is there psychotic depression?
Is there melancholic depression?
Is there atypical depression?
Is there anxious distress?
Is there mixed features?
Is there ADHD, substance use, OCD, PTSD, personality disorder or autism?
Is there hypothyroidism, anaemia, B12 deficiency, chronic inflammation, sleep apnoea, pain or medication-induced depression?
Is there suicidal risk?
Is there treatment resistance or only under-treatment?
This matters because the wrong diagnosis leads to the wrong sequence. For example, bipolar depression treated repeatedly with antidepressant monotherapy may worsen cycling, agitation or mixed states. Psychotic depression usually requires antidepressant–antipsychotic treatment or ECT. Depression with alcohol dependence will not improve fully unless alcohol use is treated. Depression with severe insomnia may need sleep-focused intervention from day one.
Step 0: Measurement-based care
One of STAR*D’s most important lessons was the value of structured follow-up. Depression should be measured, not guessed.
Useful tools include:
PHQ-9,
HAM-D,
MADRS,
GAD-7,
YMRS when bipolarity is suspected,
suicide-risk assessment,
functional assessment,
sleep and substance-use review.
The psychiatrist should document baseline severity and reassess after 2–4 weeks and again by 6–8 weeks. Response is usually defined as about 50% symptom reduction. Remission means the patient is not merely “less depressed,” but close to well.
This is important because many patients remain in a half-treated state for months: a little better, but still tired, joyless, poorly functional and cognitively dull. That is not enough.
The goal is remission and recovery, not just partial relief.
Step 1: First-line treatment for a new depressive episode
For mild depression, psychotherapy, active monitoring, exercise, sleep correction and problem-solving may be enough. For moderate to severe depression, medication, psychotherapy or a combination may be needed. NICE recommends discussing treatment options and matching them to clinical need and patient preference, with several psychological and pharmacological options available as first-line treatments for more severe depression.
Common first-line antidepressants include:
SSRIs such as escitalopram, sertraline, fluoxetine, paroxetine, fluvoxamine;
SNRIs such as venlafaxine or duloxetine;
bupropion;
mirtazapine;
vortioxetine;
agomelatine where available and appropriate;
trazodone in selected cases.
The choice depends on symptom profile.
For anxious depression: escitalopram, sertraline, paroxetine, venlafaxine or duloxetine may be considered.
For low energy and hypersomnia: bupropion, venlafaxine, duloxetine or vortioxetine may be useful.
For insomnia and weight loss: mirtazapine may help.
For prominent cognitive symptoms: vortioxetine may be considered.
For pain syndromes: duloxetine may be useful.
For sexual side-effect concern: bupropion, vortioxetine or agomelatine may be considered.
For poor appetite and sleep: mirtazapine may be a good fit.
For high suicide risk, psychosis, refusal of food or severe retardation: ECT should be considered early.
The first antidepressant should be given in an adequate dose for an adequate duration. Many “failed trials” are not true failures. They are under-dosed, stopped early, irregularly taken, or undermined by alcohol, poor sleep, medical illness or ongoing stress.
Step 2: Reassess at 2–4 weeks — early improvement matters
By 2–4 weeks, the psychiatrist should ask:
Has sleep improved?
Has anxiety reduced?
Has energy improved?
Has suicidal ideation reduced?
Are side effects tolerable?
Is the patient taking medication correctly?
Is there activation, agitation or hypomania?
Is there substance use?
Is there a psychosocial crisis maintaining symptoms?
If there is early improvement, continue and optimise. If there is no improvement at all, reconsider the diagnosis, dose, adherence and comorbidities.
A common mistake is switching too fast after 7–10 days. Another mistake is continuing the same ineffective dose for months. The correct approach is neither panic nor passivity; it is structured reassessment.
Step 3: Optimise the first antidepressant
Before declaring non-response, optimise.
This may involve:
increasing to a therapeutic dose,
waiting long enough,
managing side effects,
improving sleep,
reducing alcohol,
treating anxiety,
adding psychotherapy,
checking medical contributors,
and improving adherence.
In STAR*D level 1, citalopram was used in a structured way with dose adjustment and follow-up. Roughly one-third remitted, but many required subsequent steps.
If the patient has partial response, do not abandon a useful medicine too quickly. Partial response may be the platform for augmentation.
If there is no response, switching may be more logical.
Step 4: Switch versus augment — the key decision
After an adequate antidepressant trial, the psychiatrist has two broad options:
Switch to another antidepressant.
Augment the current antidepressant with another agent.
A simple clinical rule:
If there is no meaningful response, switch.
If there is partial response, augment or combine.
STAR*D level 2 tested both switching and augmentation strategies. Augmenting citalopram with bupropion-SR or buspirone produced similar remission rates on the primary depression scale, though bupropion had some advantages in symptom reduction and tolerability in clinical interpretation.
Modern practice has expanded augmentation options beyond STAR*D. CANMAT, NICE and VA/DoD all support structured next-step care rather than indefinite continuation of ineffective monotherapy.
Switching strategies
1. SSRI to another SSRI
This may help if the first SSRI was not tolerated or only partially effective. For example, fluoxetine to sertraline, sertraline to escitalopram, or escitalopram to fluoxetine.
Useful when:
side effects are the main issue,
the patient had some SSRI response,
anxiety is prominent,
safety and tolerability are priorities.
2. SSRI to SNRI
Switching to venlafaxine or duloxetine is common when there is poor SSRI response, prominent pain, fatigue, severe depression or anxious depression.
Venlafaxine may be useful in severe depression but needs blood pressure monitoring at higher doses. Duloxetine may be useful when depression coexists with pain, neuropathic symptoms or fibromyalgia-like complaints.
3. SSRI/SNRI to bupropion
Bupropion is useful when the clinical picture includes:
low energy, hypersomnia, poor motivation, sexual dysfunction, weight gain concern, cognitive dullness, smoking comorbidity.
It may be less ideal when anxiety, insomnia, eating disorder or seizure risk is prominent.
4. SSRI/SNRI to mirtazapine
Mirtazapine is useful when depression is associated with:
insomnia, poor appetite, weight loss, agitation, nausea, anxiety, frailty.
It may cause weight gain and sedation, which can be either helpful or problematic depending on the patient.
5. Switch to vortioxetine
Vortioxetine is a modern multimodal antidepressant with serotonergic actions. It is often considered when patients complain of cognitive symptoms, emotional blunting, sexual side effects or inadequate response to conventional SSRIs.
It is not a miracle drug, but it is a useful option in the modern depression algorithm.
Combination strategies
Combination treatment means using two antidepressants with complementary mechanisms. This is different from augmentation with lithium, antipsychotics or thyroid hormone.
1. SSRI or SNRI plus mirtazapine
This is one of the most common combinations in clinical practice.
It may help when the patient has:
partial response to SSRI/SNRI,
insomnia,
poor appetite,
weight loss,
anxiety,
residual depressive symptoms.
Mirtazapine can improve sleep and appetite while the SSRI/SNRI targets core mood and anxiety symptoms.
2. Venlafaxine plus mirtazapine: “California Rocket Fuel”
The combination of venlafaxine and mirtazapine is popularly called California Rocket Fuel, a term associated with psychopharmacologist Stephen Stahl.
The theoretical appeal is that venlafaxine enhances serotonin and noradrenaline transmission, especially at higher doses, while mirtazapine enhances noradrenergic and specific serotonergic transmission through alpha-2 antagonism and 5-HT2/5-HT3 blockade. Together, they produce a broad serotonergic–noradrenergic effect.
This combination is usually considered in more difficult depression, especially when there is:
severe depression,
insomnia,
poor appetite,
partial SNRI response,
treatment resistance,
anxious agitation with poor sleep.
However, it is not a casual first-line combination. It requires monitoring for sedation, weight gain, blood pressure, activation, drug interactions and overall tolerability.
STAR*D included venlafaxine XR plus mirtazapine at a later treatment stage, but later-stage remission rates were lower, reminding us that difficult-to-treat depression requires realistic expectations and careful follow-up.
3. SSRI/SNRI plus bupropion
This is another practical combination.
It may help when residual symptoms include:
fatigue, low motivation, hypersomnia, sexual dysfunction, poor concentration.
Bupropion can counter SSRI-related sexual dysfunction and emotional dullness in some patients. It should be used carefully in patients with severe anxiety, insomnia, seizure risk or eating disorders.
Augmentation strategies
Augmentation means adding a non-antidepressant agent to improve antidepressant response.
1. Atypical antipsychotic augmentation
Common agents include:
aripiprazole,
quetiapine XR,
brexpiprazole,
olanzapine-fluoxetine combination where available.
This strategy can be useful when there is:
partial antidepressant response,
rumination, agitation, insomnia, severe anxiety, mixed irritability, psychotic features, treatment resistance.
Aripiprazole is often activating and may help motivation, but can cause akathisia. Quetiapine can help sleep and anxiety but may cause sedation, weight gain and metabolic issues. Olanzapine has strong efficacy but significant metabolic burden.
Atypical antipsychotic augmentation is evidence-based, but it should not be used casually. Monitor weight, glucose, lipids, sedation, extrapyramidal symptoms, akathisia and prolactin depending on the agent.
2. Lithium augmentation
Lithium remains one of the classic augmentation strategies in treatment-resistant depression. It is especially important when there is suicidality, recurrent depression, bipolar-spectrum suspicion or strong family history of mood disorder.
Lithium requires:
renal function monitoring,
thyroid monitoring,
serum lithium levels,
drug-interaction review,
hydration counselling,
and toxicity education.
It is not the easiest augmentation strategy, but it is one of the most meaningful when used carefully.
3. Thyroid hormone augmentation
Triiodothyronine, or T3, has been used as an augmentation strategy, including in STAR*D later levels. It may be useful in selected patients, especially where fatigue, subclinical thyroid issues or treatment resistance are present.
It requires careful medical consideration, especially in patients with cardiac risk, osteoporosis risk or thyroid disease.
4. Buspirone augmentation
Buspirone was used in STAR*D as an augmentation option with citalopram. It may be useful when anxiety is prominent, though in current practice it is often less powerful than other augmentation strategies.
5. Stimulant or modafinil-type augmentation
In carefully selected cases with severe residual fatigue, hypersomnia or cognitive slowing, modafinil, armodafinil or stimulant-like approaches may be considered. But these are not routine depression treatments and require careful assessment for bipolarity, substance use, anxiety, cardiovascular risk and misuse potential.
Newer and advanced treatments
1. Ketamine and esketamine
Ketamine and esketamine have changed the treatment-resistant depression landscape. They are especially relevant when depression is severe, suicidal, recurrent or resistant to multiple standard treatments.
Esketamine is approved in several countries for treatment-resistant depression under supervised administration frameworks. Intravenous ketamine is used in many specialist settings, though regulatory status varies by country and protocol.
These treatments may produce rapid improvement in some patients, especially in suicidal ideation, but they require:
proper diagnosis,
blood pressure monitoring,
dissociation monitoring,
substance-use screening,
post-dose observation,
maintenance planning,
and integration with psychotherapy and standard care.
VA/DoD guidance includes ketamine/esketamine among newer options in depression care, while also noting the need for appropriate clinical selection and monitoring.
Ketamine is not a shortcut to avoid comprehensive treatment. It is an advanced tool within a structured plan.
2. rTMS
Repetitive transcranial magnetic stimulation, or rTMS, is a non-invasive brain stimulation treatment for depression. It is especially useful when patients have failed antidepressants or cannot tolerate medications.
It is generally considered when:
there is treatment-resistant depression,
medication side effects are problematic,
the patient prefers a non-systemic treatment,
there is no urgent need for ECT,
psychosis or severe suicidality is absent or controlled.
NICE includes transcranial magnetic stimulation in its depression guideline sections, and many modern algorithms place rTMS before or alongside other advanced treatments depending on availability and severity.
3. ECT
ECT remains the most effective acute treatment for severe depression, especially when there is:
suicidal intent,
psychotic depression,
refusal of food or fluids,
catatonia,
severe melancholia,
life-threatening depression,
or repeated medication failure.
ECT should not be seen as “last-stage punishment.” In the right patient, it is a rapid, life-saving treatment.
4. Light therapy
Bright light therapy is relevant not only in seasonal depression but also in selected non-seasonal depression and circadian rhythm problems. It requires care in bipolar-spectrum patients because of switch risk.
5. Digital, lifestyle and behavioural treatments
Modern depression care should also include:
sleep regularisation,
exercise prescription,
behavioural activation,
circadian rhythm stabilisation,
substance-use reduction,
nutrition,
pain management,
social rhythm therapy,
workplace modification,
and structured psychotherapy.
Medication works better when the patient’s daily life is not working against recovery.
Psychotherapy: not optional decoration
For moderate to severe, recurrent, chronic or personality-linked depression, psychotherapy is not just “counselling.” It is a core treatment.
Useful therapies include:
CBT,
behavioural activation,
interpersonal therapy,
problem-solving therapy,
mindfulness-based cognitive therapy for relapse prevention,
schema therapy where personality patterns are prominent,
trauma-focused therapy when indicated,
family interventions in selected cases.
VA/DoD recommends psychotherapy or pharmacotherapy as monotherapy based on patient preference in many cases, and suggests combination pharmacotherapy plus evidence-based psychotherapy for severe, persistent or recurrent major depressive disorder.
The psychotherapy target depends on the depression subtype.
For rumination: CBT and metacognitive approaches.
For withdrawal: behavioural activation.
For grief and role transitions: interpersonal therapy.
For chronic low self-worth: schema-focused work.
For trauma-linked depression: trauma-informed care.
For recurrent relapse: mindfulness-based cognitive therapy.
A practical modern STAR*D-style algorithm
Stage 1: Diagnose and start first-line treatment
Confirm unipolar depression.
Assess suicide risk and bipolarity.
Start SSRI/SNRI/bupropion/mirtazapine/vortioxetine depending on profile.
Add psychotherapy where possible.
Correct sleep, alcohol, medical issues and adherence.
Stage 2: Optimise
At 2–4 weeks, assess early change.
At 6–8 weeks, decide whether response is adequate.
Increase dose if tolerated and partially effective.
Manage side effects actively.
Stage 3: Switch or augment
If no response: switch class.
If partial response: augment or combine.
Options include bupropion add-on, mirtazapine add-on, SNRI switch, vortioxetine switch, aripiprazole/quetiapine augmentation, lithium, T3 or psychotherapy intensification.
Stage 4: Treat difficult-to-treat depression
Reassess diagnosis.
Check bipolarity, ADHD, trauma, substance use, personality disorder, sleep apnoea, thyroid, B12, pain, inflammation, medications.
Consider California Rocket Fuel, atypical antipsychotic augmentation, lithium, rTMS, ketamine/esketamine, or ECT depending on severity and risk.
Stage 5: Recovery and relapse prevention
Continue medication after remission.
Treat residual symptoms.
Build relapse signature.
Add psychotherapy for recurrence prevention.
Plan taper only after stability and risk review.
How long should treatment continue?
Stopping too early is one of the commonest reasons for relapse.
A first depressive episode usually requires continuation treatment for several months after remission. Recurrent depression, severe depression, chronic depression, psychotic depression or depression with suicidality often requires longer maintenance.
The question is not, “Can I stop once I feel better?”
The better question is:
“How do we consolidate recovery so that I do not fall back?”
Patients should be taught their relapse signature:
sleep disturbance,
early morning waking,
loss of interest,
social withdrawal,
irritability,
negative thinking,
fatigue,
loss of routine,
increased alcohol use,
suicidal thoughts.
Early relapse detection prevents full relapse.
Why treatment-resistant depression should be re-formulated, not just medicated
When two adequate antidepressant trials fail, the psychiatrist should pause and re-formulate.
Ask:
Is this actually bipolar depression?
Is there mixed anxiety and agitation?
Is there undiagnosed ADHD?
Is there autism with burnout?
Is there alcohol or cannabis use?
Is there sleep apnoea?
Is there chronic pain?
Is there hypothyroidism, B12 deficiency or anaemia?
Is there personality disorder or trauma?
Is there ongoing domestic conflict?
Is the patient taking the medicine properly?
Is the dose adequate?
Is the patient seeking symptom relief but living in the same toxic rhythm?
Treatment resistance is often not just pharmacological resistance. It is a signal that the case needs deeper understanding.
Patient-friendly summary
Depression treatment usually follows a stepwise plan.
First, confirm the diagnosis and severity.
Second, start a suitable antidepressant or psychotherapy.
Third, measure response using tools like PHQ-9.
Fourth, optimise dose and duration.
Fifth, if response is poor, switch or augment.
Sixth, if depression is resistant, consider combinations such as SSRI/SNRI plus mirtazapine, venlafaxine plus mirtazapine, bupropion add-on, lithium, atypical antipsychotic augmentation, ketamine/esketamine, rTMS or ECT.
Finally, continue treatment long enough to prevent relapse.
STAR*D taught us that many patients need more than one step. Modern psychiatry adds more refined steps, better measurement, newer medicines, psychotherapy, brain stimulation and personalised treatment planning.
The aim is not just to reduce sadness.
The aim is remission, recovery, functioning and relapse prevention.
Conclusion
A sophisticated depression treatment plan is not a single prescription. It is a sequence.
Diagnose correctly.
Measure severity.
Treat adequately.
Optimise before abandoning.
Switch when there is no response.
Augment when there is partial response.
Use combinations thoughtfully.
Consider newer agents and brain-based treatments when needed.
Continue treatment after remission.
Prevent relapse.
STAR*D showed that depression often requires persistence and sequencing. Modern guidelines now allow us to go further: to personalise treatment based on symptoms, side effects, cognition, sleep, suicidality, comorbidity, patient preference and treatment history.
Depression is treatable, but it must be treated systematically.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808