The Brain’s “Inner World” Network: Why the Default Mode Network Matters in Psychiatry
 Introduction: The Brain Is Never Truly Silent
Introduction: The Brain Is Never Truly Silent
For a long time, we believed that the brain was most active only when it was solving problems, reading, calculating, speaking, or responding to the outside world. Rest was assumed to be a kind of biological pause.
Modern neuroscience changed that view dramatically.
When the brain is not focused on an external task, a powerful internal network becomes active. This network is called the Default Mode Network, or DMN. It is involved in self-reflection, memory, imagination, emotional processing, social understanding, and the construction of our personal life story. In simple terms, the DMN is the brain system that becomes active when the mind turns inward.
It is the network behind thoughts such as:
“Why did I react like that?”
“What will happen tomorrow?”
“What does that person think of me?”
“Why do I keep remembering that incident?”
“What kind of person am I becoming?”
This makes the DMN deeply relevant to psychiatry. Many psychiatric symptoms are not only about mood, anxiety, or behavior. They are also about the way the person relates to the self, remembers the past, anticipates the future, interprets others, and regulates internal mental noise.
That is exactly where the DMN becomes important.
What Is the Default Mode Network?
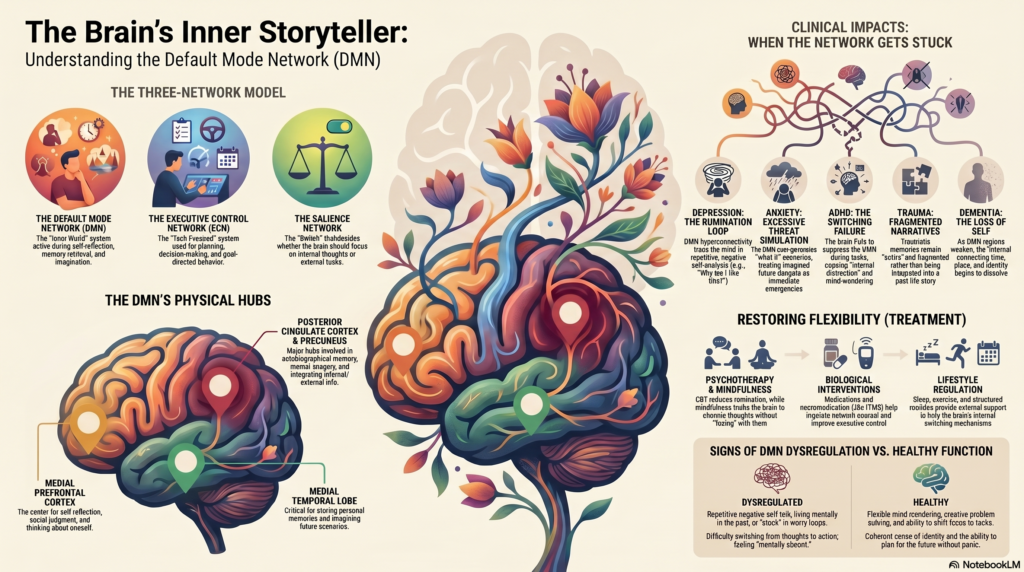
The Default Mode Network is a large-scale brain network that shows synchronized activity during rest, daydreaming, mind-wandering, autobiographical memory, and self-referential thinking. It was identified through neuroimaging studies, especially functional MRI, which showed that certain brain regions become more active when a person is not engaged in a specific external task.
The key regions commonly associated with the DMN include:
- Medial prefrontal cortex
Involved in self-reflection, emotional meaning, social judgment, and thinking about oneself. - Posterior cingulate cortex
A major hub of the DMN, involved in self-related processing, autobiographical memory, and integration of internal and external information. - Precuneus
Involved in mental imagery, memory retrieval, perspective-taking, and imagining future scenarios. - Inferior parietal lobule
Helps integrate sensory, cognitive, and social information. - Medial temporal lobe and hippocampal connections
Important for autobiographical memory and imagining future events. - Orbitofrontal and limbic connections
Link the DMN with emotion, reward, decision-making, and meaning.
The DMN is not a single “button” in the brain. It is better understood as a network of interacting regions that help us create an internal model of ourselves and the world.
The DMN as the Brain’s Inner Storyteller
One of the most clinically useful ways to understand the DMN is to think of it as the brain’s inner storyteller.
It helps us connect past, present, and future. It allows us to remember our childhood, understand our present emotional state, and imagine what may happen next. It gives continuity to the self.
Without this network, life would feel like disconnected moments. With it, we are able to say:
“This happened to me.”
“This is how it affected me.”
“This is what I fear.”
“This is what I hope for.”
“This is who I am.”
The DMN therefore contributes to identity formation, autobiographical memory, and personal meaning. This is why it is so relevant in depression, anxiety, trauma, personality disorders, addiction, ADHD, autism, schizophrenia, and dementia.
Psychiatry is not only about symptoms. It is also about the narrative structure of the mind. The DMN is one of the neural systems that helps build that narrative.
The DMN and the Three-Network Model of the Mind
The DMN does not work alone. It interacts with other major brain networks, especially the Executive Control Network and the Salience Network.
1. Default Mode Network: the inner world
The DMN is active during self-reflection, memory, imagination, and internally focused thought.
2. Executive Control Network: the task-focused system
This network helps with planning, working memory, decision-making, impulse control, and goal-directed behavior.
3. Salience Network: the switch
The Salience Network detects what is important. It decides whether the brain should stay in internal reflection or shift attention to the outside world. It helps switch between the DMN and executive networks.
In a healthy brain, these systems work flexibly. When we need to focus, the DMN quietens and the Executive Control Network becomes more active. When we rest or reflect, the DMN becomes active again.
But in many psychiatric conditions, this switching becomes inefficient. The person may remain trapped in rumination, worry, intrusive memories, self-criticism, dissociation, or mental noise. The uploaded review highlights that the Salience Network acts like a switch between the DMN and Executive Control Network, helping the brain prioritize important information and regulate emotional states.
When the DMN Becomes Too Loud: Rumination and Depression
In depression, the mind often becomes painfully self-focused.
The person may repeatedly think:
“Why am I like this?”
“I have failed.”
“Nothing will change.”
“Everyone is better than me.”
“My past mistakes define me.”
This is not ordinary reflection. It is rumination — repetitive, negative, self-focused thinking that does not lead to problem-solving.
DMN hyperconnectivity or abnormal DMN regulation has been linked to depressive rumination. The posterior cingulate cortex and medial prefrontal cortex are particularly important because they are involved in self-referential thinking and emotional meaning. When these systems become overactive or poorly regulated, the person may get stuck in a loop of negative self-analysis.
Clinically, this explains why depressed patients may say:
“My mind does not stop.”
“I know I should not think like this, but I keep going back to the same thoughts.”
“I cannot move on from the past.”
“I am constantly judging myself.”
From a DMN perspective, depression is not just low mood. It is also a disorder of self-processing, memory bias, and future prediction. The depressed brain often retrieves painful memories, interprets the self harshly, and imagines the future pessimistically.
This is why treatments that reduce rumination — such as cognitive behavior therapy, behavioral activation, mindfulness-based therapies, antidepressants, sleep correction, exercise, and neuromodulation — may help by restoring better balance between the DMN, executive control systems, and emotional networks.
Anxiety: When the DMN Simulates Threats
Anxiety is often future-oriented.
The anxious mind asks:
“What if something goes wrong?”
“What if I fail?”
“What if I lose control?”
“What if people judge me?”
“What if this symptom means something serious?”
The DMN helps simulate future scenarios. This is useful when planning. But when this capacity becomes excessive and threat-focused, it may contribute to worry.
In anxiety disorders, the brain may repeatedly create imagined future dangers. The person is not only reacting to real threats but also to internally generated simulations of threat. The DMN works with the amygdala, prefrontal cortex, and salience systems to attach emotional significance to these imagined possibilities.
This helps us understand why reassurance often works only briefly. The person is not only afraid of one situation. The brain keeps generating new “what if” scenarios.
Therapy, therefore, should not merely provide reassurance. It should help the person change their relationship with internal predictions.
Useful interventions include:
Cognitive restructuring, worry postponement, exposure therapy, interoceptive exposure, mindfulness, relaxation training, sleep regulation, and reducing avoidance behaviors.
The goal is not to stop thinking. The goal is to prevent the mind from treating every imagined future as an emergency.
Trauma and PTSD: When the Past Refuses to Become Past
In trauma-related conditions, the DMN becomes clinically important because trauma affects autobiographical memory, self-identity, emotional regulation, and the sense of safety.
A traumatic memory is not just a memory. It can become a living internal state.
The person may feel:
“It is happening again.”
“I am not safe.”
“I am permanently damaged.”
“I cannot trust people.”
“My life is divided into before and after.”
The DMN is involved in autobiographical memory and self-narrative. Trauma can disturb the way memories are integrated into the life story. Instead of being stored as “something that happened,” the traumatic experience may remain emotionally active, fragmented, intrusive, or shame-laden.
This is why trauma therapy often focuses on integration.
The aim is not to erase the memory. The aim is to help the brain place the memory in time, reduce its emotional charge, and rebuild a coherent sense of self.
Approaches such as trauma-focused CBT, EMDR, prolonged exposure, narrative exposure therapy, compassion-focused therapy, and body-based regulation strategies may help by changing the relationship between memory, emotion, and self-representation.
ADHD: Difficulty Switching From Inner Noise to Task Focus
ADHD is usually described in terms of attention, impulsivity, hyperactivity, and executive dysfunction. But the DMN gives us another elegant way to understand ADHD.
In ADHD, one problem may be poor suppression of the DMN during tasks.
When a student is trying to read, the brain should shift from mind-wandering to task-focused attention. But if the DMN intrudes into the task state, the mind drifts.
The person may experience:
“I read the same paragraph again and again.”
“My mind goes somewhere else.”
“I start one task and end up doing another.”
“I know what to do, but I cannot stay with it.”
“I am physically present, but mentally absent.”
This is not laziness. It may reflect unstable switching between the DMN and executive attention networks.
In ADHD, mind-wandering is often not pleasant creativity. It is uncontrolled internal distraction. The person may lose time, forget instructions, postpone tasks, or struggle with consistency.
This also explains why structure helps. External structure reduces the burden on internal control networks. Timers, visual schedules, accountability, environmental modification, medication, sleep correction, and behavioral strategies can help the brain stay engaged with the task.
In clinical language, ADHD may be partly understood as a disorder of network regulation — especially the ability to suppress irrelevant internal mentation when external performance is required.
Autism: The DMN and Social Meaning
The DMN is also involved in social cognition — the ability to understand other people’s thoughts, intentions, emotions, and perspectives.
This is relevant in autism spectrum conditions. Some individuals with autism may have differences in how social information is processed, how mental states are inferred, and how self-other boundaries are represented.
This does not mean autistic individuals lack emotion or empathy. That is an outdated and inaccurate stereotype. Rather, the neural systems involved in social prediction, sensory integration, self-reflection, and social interpretation may work differently.
The DMN’s role in theory of mind, autobiographical memory, and social understanding makes it a useful framework for thinking about autism. It may help explain why some autistic individuals find social situations mentally exhausting, unpredictable, or ambiguous.
Clinical care should therefore move beyond forcing superficial social behavior. A better approach is to support communication, sensory regulation, emotional literacy, predictable routines, strengths, autonomy, and meaningful social participation.
Schizophrenia and Psychosis: When Internal Models Become Too Powerful
In psychosis, the boundary between internally generated meaning and external reality may become disturbed.
The DMN may be relevant here because it is involved in self-referential thinking, internal mentation, memory, and meaning-making. If internal thoughts, associations, or salience signals become dysregulated, the person may begin to experience private meanings as externally significant.
For example:
A neutral event may feel personally directed.
A random sound may feel like a message.
A thought may feel inserted or controlled.
An internal fear may become a fixed belief.
The DMN alone does not “cause” psychosis. Psychosis involves multiple systems — dopamine salience, sensory prediction, executive control, memory, trauma, and social cognition. But the DMN offers a helpful way to understand why self-referential meaning becomes so central in psychotic experiences.
Treatment needs to reduce distress, restore sleep, regulate salience, improve reality testing, support cognition, and rebuild social functioning. Medication, psychoeducation, family work, CBT for psychosis, occupational rehabilitation, and relapse prevention all have a role.
Dementia and Alzheimer’s Disease: When the Network of Memory Weakens
The DMN overlaps with regions vulnerable in Alzheimer’s disease, especially areas involved in memory and self-referential processing. The posterior cingulate cortex, precuneus, and medial temporal lobe connections are particularly important.
This may explain why early dementia is not only about forgetting names or misplacing objects. It is also about disruption in the continuity of self.
Families may say:
“He is not the same person.”
“She has lost interest in things she loved.”
“He forgets recent events but remembers old stories.”
“She becomes confused in familiar situations.”
The DMN helps integrate memory, identity, and orientation. When this network becomes disrupted, the person may lose not only information but also the smooth internal map that connects time, place, person, and meaning.
This has practical implications. Dementia care should include not only memory medicines and cognitive screening but also routine, emotional familiarity, autobiographical cues, meaningful activities, caregiver education, sleep correction, sensory optimization, and management of depression or anxiety.
Addiction: The DMN, Craving, and the Remembered Self
Addiction is not just a habit. It is a disorder of reward, memory, stress, identity, and future prediction.
The DMN may contribute to addiction through craving-related memory, self-narrative, and imagined relief.
The person may think:
“Only this will calm me.”
“I cannot function without it.”
“I have already failed, so why try?”
“I will quit tomorrow.”
“One last time.”
Craving is often strengthened by autobiographical memory and emotional prediction. The brain remembers relief, anticipates comfort, and minimizes consequences. The DMN may participate in this internal simulation.
Recovery therefore requires more than detoxification. It requires rebuilding the self-story.
The person has to move from:
“I am an addict and I cannot change”
to
“I am a person recovering, one decision at a time.”
Psychotherapy, relapse prevention, medication-assisted treatment, family support, sleep restoration, routine, peer support, and meaning-based recovery can help reshape the internal narrative.
Personality Disorders: The DMN and the Sense of Self
Personality disorders often involve difficulties in identity, emotional regulation, interpersonal interpretation, and self-other boundaries. These are deeply connected to DMN functions.
In borderline personality organization, for example, the person may experience rapid shifts in self-state:
“I am good.”
“I am bad.”
“They love me.”
“They will abandon me.”
“I cannot tolerate this feeling.”
“My life has no stable center.”
The DMN contributes to self-continuity. When self-representations are unstable, emotionally overloaded, or trauma-linked, the internal narrative becomes fragmented.
This is why therapies such as DBT, mentalization-based therapy, schema therapy, transference-focused psychotherapy, and supportive psychodynamic therapy are so relevant. They help patients observe internal states, name emotions, understand interpersonal meanings, and build a more stable self-narrative.
From a network perspective, therapy is not just “talk.” It is repeated training in emotional regulation, perspective-taking, autobiographical integration, and reflective functioning.
The DMN in Childhood and Adolescence
The DMN matures through childhood and adolescence. This is important because the developing brain is highly sensitive to environment, attachment, education, stress, and trauma.
Healthy DMN development supports:
Self-awareness
Emotional regulation
Autobiographical memory
Social understanding
Future planning
Identity formation
Adverse childhood experiences, chronic stress, neglect, abuse, poverty, unstable caregiving, and poor emotional support can affect the maturation of networks involved in self-regulation and emotional processing. The uploaded review emphasizes that childhood adversity can alter DMN maturation and connectivity, with possible long-term implications for depression, PTSD, anxiety, interpersonal difficulties, and overall well-being.
This is clinically important. Childhood mental health care is not only symptom control. It is brain development support.
Good parenting, predictable routines, emotional validation, play, education, sleep, nutrition, physical activity, and early psychological intervention may all help build healthier network regulation.
Mind-Wandering: Problem or Gift?
Mind-wandering is not always pathological.
The DMN supports creativity, imagination, autobiographical reflection, and future planning. Many insights occur when the mind is not tightly focused. A walk, a shower, a quiet moment, or a relaxed conversation may allow the DMN to connect ideas in new ways.
The problem is not mind-wandering itself. The problem is loss of flexibility.
Healthy DMN function allows the mind to move inward and outward as needed.
Unhealthy DMN regulation traps the person in:
Rumination
Worry
Intrusive memories
Self-criticism
Daydreaming without action
Dissociation
Craving
Suspicious meaning-making
Negative future simulation
Mental health depends not on silencing the inner world, but on regulating it.
Can We Measure the DMN Clinically?
The DMN is usually studied using research tools such as:
Functional MRI
Resting-state functional connectivity analysis
EEG
MEG
PET
Diffusion imaging
Computational network analysis
The uploaded review notes that fMRI has high spatial resolution and is useful for mapping resting-state connectivity, while EEG and MEG offer better temporal resolution for capturing rapid neural activity. PET can study metabolism but is more invasive.
In routine psychiatric practice, we do not diagnose depression, ADHD, anxiety, or schizophrenia by “checking the DMN” directly. However, DMN research is shaping the future of psychiatry.
It may help us develop:
Better biomarkers
More precise treatment selection
Neurofeedback protocols
Personalized neuromodulation
Cognitive training models
Early risk markers
Better understanding of psychotherapy mechanisms
The future of psychiatry may increasingly involve network-based formulations, where symptoms are understood through disrupted coordination between brain systems.
How Treatments May Influence the DMN
Many psychiatric treatments may work partly by improving network flexibility.
1. Psychotherapy
CBT can reduce rumination, restructure negative beliefs, and improve cognitive control over repetitive self-focused thinking.
Mindfulness helps people observe thoughts without becoming fused with them. This may reduce excessive DMN dominance and improve present-moment awareness.
Psychodynamic therapy may help reorganize autobiographical memory, self-narrative, and relational patterns.
DBT and mentalization-based therapies improve self-observation, emotional regulation, and interpersonal understanding.
2. Medication
Antidepressants, stimulants, antipsychotics, mood stabilizers, and anxiolytic strategies may indirectly affect DMN functioning by changing mood, arousal, salience, sleep, cognition, and emotional reactivity.
For example, ADHD medication may help reduce task-irrelevant mind-wandering by improving executive control. Antidepressants may reduce negative rumination by improving mood regulation and cognitive-emotional flexibility.
3. Neuromodulation
rTMS, tDCS, neurofeedback, and other neuromodulation approaches may increasingly target large-scale networks rather than isolated symptoms.
For example, stimulation of prefrontal regions may influence executive control, mood regulation, and DMN interactions.
4. Lifestyle interventions
Sleep, exercise, meditation, social connection, structured routine, sunlight exposure, and reduced substance use can all influence brain network regulation.
Good psychiatry should not separate biology from lifestyle. The brain’s networks are shaped every day by behavior, environment, relationships, and meaning.
A Clinical Way to Explain the DMN to Patients
For patient education, the DMN can be explained simply:
“Your brain has an inner-world network. It helps you remember, reflect, imagine, and understand yourself. But when you are stressed, depressed, anxious, sleep-deprived, traumatized, or overwhelmed, this network can become overactive or poorly regulated. Then the mind gets stuck in loops — worry loops, guilt loops, fear loops, craving loops, or self-doubt loops. Treatment helps your brain regain flexibility, so you can shift from inner noise to meaningful action.”
This explanation is often validating. It helps patients understand that they are not “weak” or “overthinking by choice.” Their brain is stuck in a pattern — and patterns can be changed.
Practical Signs of DMN Dysregulation in Daily Life
A person may be struggling with DMN-related difficulties if they frequently experience:
Repetitive negative self-talk
Excessive daydreaming
Difficulty staying on task
Persistent worry about the future
Living mentally in the past
Intrusive autobiographical memories
Overinterpretation of others’ behavior
Difficulty switching from thoughts to action
Feeling trapped in guilt or shame
Uncontrolled craving-related thinking
Poor emotional recovery after stress
Loss of sense of self or direction
These are not diagnostic by themselves, but they are useful clinical clues.
What Patients Can Do to Regulate the Inner Network
Some simple strategies can help reduce excessive internal looping:
1. Name the loop
Instead of saying, “This is true,” say, “My mind is running a worry loop” or “This is rumination.”
2. Shift from thinking to doing
Behavioral activation helps because action recruits task-focused networks.
3. Use external structure
Calendars, checklists, timers, visual reminders, and accountability reduce dependence on internal control.
4. Practice mindful observation
The aim is not to stop thoughts but to see them as mental events.
5. Improve sleep
Sleep deprivation worsens emotional reactivity, attention, and internal mental noise.
6. Move the body
Exercise improves mood, cognition, and network flexibility.
7. Reduce avoidance
Avoidance strengthens fear simulations. Gradual exposure teaches the brain that imagined danger is not always real danger.
8. Build meaningful social connection
The DMN is also a social brain network. Safe relationships help reorganize the internal self-story.
The Future: Toward Network-Based Psychiatry
Psychiatry is gradually moving from a purely symptom-based model toward a more integrated model involving brain networks, development, cognition, emotion, trauma, social context, and personal meaning.
The DMN is central to this transition.
It helps us connect neuroscience with lived experience.
Depression becomes more than sadness.
It becomes a disorder of negative self-narrative and rumination.
Anxiety becomes more than fear.
It becomes excessive future simulation and threat prediction.
ADHD becomes more than distractibility.
It becomes difficulty regulating the shift between internal and external attention.
Trauma becomes more than memory.
It becomes a disruption in autobiographical integration and safety prediction.
Addiction becomes more than craving.
It becomes a remembered, embodied, self-reinforcing narrative of relief.
This is where modern psychiatry becomes both scientific and humane.
The brain is not just a chemical organ. It is a meaning-making organ.
Conclusion: Healing the Brain’s Inner Conversation
The Default Mode Network is one of the most important discoveries in modern neuroscience because it gives us a biological window into the inner life.
It helps explain why humans remember, imagine, regret, hope, worry, create, grieve, love, and search for meaning.
In mental health, suffering often begins when the inner world becomes rigid, threatening, repetitive, or disconnected from reality. Healing begins when the brain regains flexibility — the ability to reflect without drowning, remember without reliving, plan without panicking, and act without being trapped by inner noise.
The future of psychiatry will not be only about reducing symptoms. It will be about restoring healthy brain network dynamics, rebuilding coherent self-narratives, and helping people move from survival loops to meaningful living.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery Opp. Phoenix Mall
✉ srinivasaiims@gmail.com 📞 +91-8595155808