Role of a Psychiatrist in Dementia Management
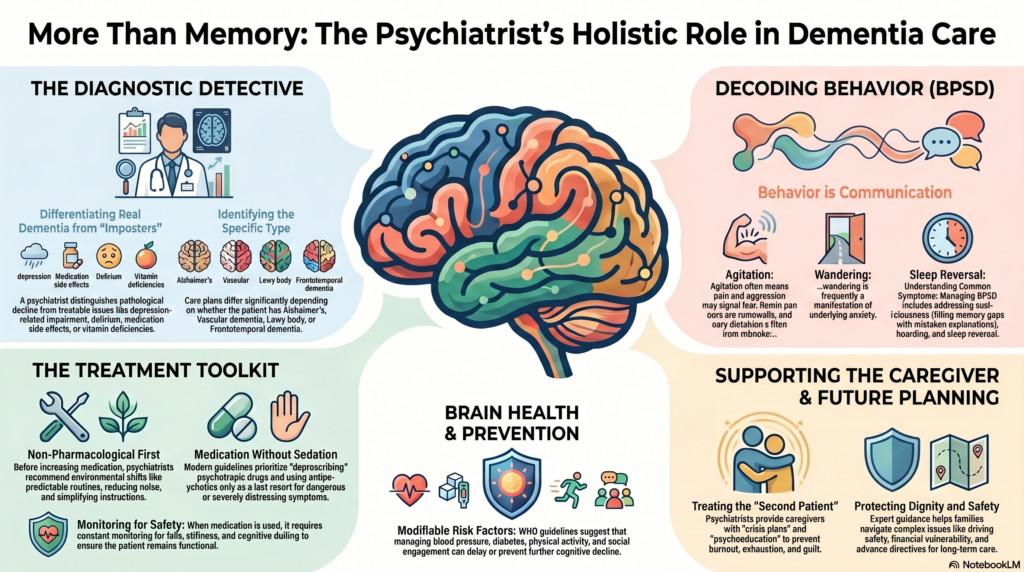 A psychiatrist has a central role in dementia care because dementia is not only a memory disorder. It affects mood, behaviour, sleep, judgement, personality, family relationships, safety and caregiver wellbeing. In many patients, the most distressing part of dementia is not forgetfulness itself, but agitation, suspiciousness, depression, aggression, wandering, hallucinations, sleep reversal or caregiver burnout.
A psychiatrist has a central role in dementia care because dementia is not only a memory disorder. It affects mood, behaviour, sleep, judgement, personality, family relationships, safety and caregiver wellbeing. In many patients, the most distressing part of dementia is not forgetfulness itself, but agitation, suspiciousness, depression, aggression, wandering, hallucinations, sleep reversal or caregiver burnout.
A good dementia psychiatrist helps the family move from the question “Is this dementia?” to a more useful question:
“What type of neurocognitive dysfunction is this, what is reversible, what needs treatment, and how do we preserve dignity and function?”
1. Differentiating dementia from other psychiatric and medical conditions
Many elderly patients are labelled as having dementia when the actual problem may be depression, delirium, sleep disturbance, medication side effects, alcohol use, vitamin deficiency, thyroid disorder or sensory impairment.
A psychiatrist helps differentiate:
Normal aging from pathological cognitive decline
Depression-related cognitive impairment from dementia
Delirium from dementia
Mild cognitive impairment from established dementia
Alzheimer’s disease from vascular dementia, Lewy body dementia, frontotemporal dementia and Parkinson’s disease dementia
Medication-induced cognitive dulling from primary neurodegeneration
This distinction is crucial because some causes are treatable or partially reversible.
2. Assessing behavioural and psychological symptoms of dementia
The psychiatrist’s most important role is often in managing BPSD — behavioural and psychological symptoms of dementia.
These include:
agitation, aggression, irritability, suspiciousness, delusions, hallucinations, sleep reversal, wandering, apathy, depression, anxiety, disinhibition, repetitive questioning, hoarding, refusal of care and sexually inappropriate behaviour.
Modern guidelines emphasise structured assessment and management of BPSD, including agitation, depression, anxiety, psychosis, sexual expressions of risk, and deprescribing psychotropic medication when possible.
The key psychiatric principle is:
Behaviour is often communication.
Agitation may mean pain.
Aggression may mean fear.
Wandering may mean anxiety.
Refusal to bathe may mean loss of sequencing, sensory discomfort or embarrassment.
Suspiciousness may arise because memory gaps are being filled with mistaken explanations.
The psychiatrist helps the family decode these behaviours instead of simply suppressing them.
3. Careful use of psychiatric medication
Medication has a role, but dementia care should not become careless sedation.
A psychiatrist decides when medication is truly needed for:
severe depression, anxiety, insomnia, psychosis, aggression, agitation, disinhibition or dangerous behaviour.
Medicines may include antidepressants, sleep-regulating strategies, cholinesterase inhibitors, memantine, or carefully selected antipsychotics in severe cases.
However, antipsychotics in dementia require caution. NICE recommends psychosocial and environmental interventions to reduce antipsychotic need, dose reduction where possible, freedom of movement, and minimising restraint.
A psychiatrist’s role is therefore not just to prescribe, but to ask:
Is medication needed?
Is the symptom dangerous or severely distressing?
Can pain, infection, constipation, sleep disturbance or caregiver interaction explain the behaviour?
Can the dose be reduced later?
Are we monitoring sedation, falls, stiffness, stroke risk and cognition?
4. Managing depression, anxiety and apathy in dementia
Depression and anxiety are common in dementia and may worsen memory, motivation, sleep and daily functioning. Sometimes the first presentation of dementia is not memory loss but withdrawal, fearfulness, irritability or loss of interest.
The psychiatrist evaluates whether the patient has:
major depression, anxiety disorder, grief, adjustment difficulty, apathy due to frontal-subcortical dysfunction, or emotional distress related to awareness of decline.
This matters because depression is treatable, and treating it may improve quality of life, cooperation with care and family interaction.
5. Supporting caregivers and reducing burnout
Dementia is a family illness. The caregiver often becomes the “second patient.”
Caregivers may experience exhaustion, guilt, anger, helplessness, insomnia, financial strain, sibling conflict and anticipatory grief.
A psychiatrist helps caregivers by providing:
psychoeducation, behaviour management strategies, crisis plans, communication techniques, sleep routines, medication supervision plans, safety guidance, and realistic expectations about disease progression.
This is one of the most valuable parts of dementia psychiatry. A calm, informed caregiver can often reduce the patient’s distress more effectively than medication.
6. Building a non-pharmacological behaviour plan
Before increasing tablets, the psychiatrist often works with the family on environmental and behavioural modification.
Examples include:
maintaining a predictable daily routine, reducing overstimulation, avoiding repeated correction, simplifying instructions, improving lighting, reducing noise, using memory cues, preventing evening confusion, improving sleep hygiene, managing pain and constipation, ensuring hearing aids or glasses are used, and creating safe walking spaces.
NICE dementia guidance highlights training and support for staff and carers to understand and respond to agitation, aggression, pain and other behaviours indicating distress.
7. Risk reduction and brain-health planning
The psychiatrist also helps with dementia prevention and progression modification. WHO guidelines on risk reduction of cognitive decline and dementia recommend evidence-based lifestyle and health interventions to delay or prevent cognitive decline.
This includes attention to:
physical activity, smoking cessation, alcohol reduction, blood pressure control, diabetes control, dyslipidaemia management, weight optimisation, sleep, depression treatment, social engagement and cognitive stimulation.
In Indian families, this approach is especially important because vascular risk factors, sleep problems, polypharmacy and untreated depression often worsen cognition.
8. Coordinating care with neurology, medicine and family physicians
Dementia care is multidisciplinary. A psychiatrist works alongside neurologists, physicians, geriatricians, psychologists, occupational therapists, speech therapists and social workers.
The psychiatrist is particularly useful when the clinical picture includes:
behavioural disturbance, psychosis, depression, anxiety, sleep reversal, caregiver distress, personality change, disinhibition, addiction, medication complexity or decision-making concerns.
In frontotemporal dementia, Lewy body dementia and vascular cognitive impairment, psychiatric symptoms may dominate the clinical picture. Here, psychiatric expertise becomes even more important.
9. Helping families with capacity, safety and future planning
Dementia gradually affects judgement and decision-making. A psychiatrist helps families think through:
financial safety, driving safety, medication supervision, wandering risk, home safety, consent capacity, vulnerability to exploitation, advance directives, caregiver succession and long-term care planning.
This is not merely administrative. It protects the patient’s dignity and reduces future crises.
10. Preserving dignity
The deepest role of the psychiatrist is to help families see the person behind the illness.
A patient with dementia is not “behaving badly.”
They are living with a changing brain.
They may be frightened, confused, ashamed or overwhelmed.
The family needs both science and compassion.
The psychiatrist brings together diagnosis, medication, behavioural science, caregiver counselling and long-term planning into one coherent care model.
Summary
A psychiatrist helps in dementia by:
diagnosing the type and stage of cognitive decline,
identifying reversible causes,
treating depression, anxiety, sleep problems and psychosis,
managing agitation and aggression safely,
reducing unnecessary sedation,
guiding caregivers,
planning home-based behavioural strategies,
coordinating with other specialists,
and preserving dignity and quality of life.
Dementia management is not just about memory tablets. It is about helping the patient and family live better with a complex brain disorder.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Dementia Series: The Role of Technology in Dementia Care – Innovations for Better Support
- Dementia Series: Young-Onset Dementia – When Dementia Strikes Early
- Behavioral and Psychological Symptoms of Dementia(BPSD) Management
- Technology in Dementia Management: A Modern Approach
- Perimenopausal Disorders: The Crucial Role of the Psychiatrist
- The Role of the Psychiatrist in Parkinsonism: Beyond Movement Control