Diabetes and Mental Health: Why Sugar Control Is Not Just About Sugar
 Diabetes is usually discussed in numbers: fasting sugar, post-meal sugar, HbA1c, cholesterol, weight, and blood pressure. But anyone living with diabetes knows that the condition is not only biological. It is also emotional.
Diabetes is usually discussed in numbers: fasting sugar, post-meal sugar, HbA1c, cholesterol, weight, and blood pressure. But anyone living with diabetes knows that the condition is not only biological. It is also emotional.
A major 2026 review in The Lancet Diabetes & Endocrinology highlights five mental health challenges commonly seen in people with type 1 diabetes, type 2 diabetes, and gestational diabetes: fear of low sugar, diabetes distress, depression, disordered eating, and sleep problems. These issues can reduce quality of life, affect self-care, worsen HbA1c, and increase long-term health risks.
1. Fear of low sugar
People taking insulin or certain diabetes medicines may fear hypoglycaemia — sudden drops in blood glucose. This fear is understandable. A low-sugar episode can cause sweating, shaking, confusion, weakness, palpitations, or even loss of consciousness.
But when fear becomes excessive, people may start keeping their sugar deliberately high, avoiding exercise, eating extra “just in case,” or checking sugar repeatedly. This gives temporary emotional safety but may harm long-term control.
The answer is not to dismiss the fear. The answer is to make diabetes safer: review medicines, learn hypoglycaemia correction, use glucose monitoring when appropriate, and discuss fear openly with the doctor.
2. Diabetes distress
Diabetes distress is not the same as depression. It is the emotional exhaustion of managing a condition that never takes a holiday.
It sounds like:
“I am tired of checking sugars.”
“I know what to do, but I cannot keep doing it every day.”
“Everyone blames me for my sugar.”
“I feel guilty whenever I eat.”
“I am scared of future complications.”
This distress is common because diabetes demands constant decision-making: what to eat, when to exercise, whether to take medicines, how to handle festivals, travel, work stress, infections, and family pressure. A 2024 International Diabetes Federation survey found that many people with diabetes reported anxiety, depression, burnout, stigma, fear of complications, and a desire for more emotional support from healthcare providers.
3. Depression and diabetes
Depression can reduce motivation, energy, sleep, concentration, appetite regulation, and hope. In diabetes, this can directly affect medicine adherence, diet, physical activity, appointments, and glucose monitoring.
The relationship works both ways. Diabetes can increase emotional burden, and untreated mental health problems can make diabetes harder to manage. The CDC notes that people with diabetes are more likely to have depression, and that mental health problems and diabetes can worsen each other.
Depression in diabetes should not be mistaken for “laziness” or “lack of discipline.” It is a treatable medical condition.
4. Disordered eating
Diabetes can make food emotionally complicated. Some people become overly restrictive. Some binge after prolonged control. Some feel shame after eating sweets. In type 1 diabetes, some may even misuse insulin to influence weight, which can be dangerous.
The goal is not fear-based eating. The goal is a sustainable relationship with food: structured meals, realistic portions, flexibility, and freedom from guilt.
A person with diabetes should not have to live with the feeling that every meal is an exam.
5. Sleep problems
Poor sleep affects appetite, cravings, mood, insulin resistance, and daytime energy. Diabetes can disturb sleep through frequent urination, nocturnal hypoglycaemia, neuropathic pain, restless legs, obstructive sleep apnoea, anxiety, or depression.
When sleep improves, diabetes care often becomes easier. Sleep should be routinely asked about in diabetes consultations, not treated as a side issue.
What actually helps?
The good news is that psychological interventions can help. The Lancet review notes evidence for approaches such as cognitive behavioural therapy, mindfulness-based cognitive therapy, stepped care, and digital psychological support, especially for short-term symptom reduction. But it also cautions that diabetes-related emotional problems can recur, so ongoing support matters.
Practical support may include:
- Screening for depression, anxiety, sleep problems, diabetes distress, and eating concerns.
- Reviewing medicines if hypoglycaemia fear is high.
- Simple behavioural plans instead of unrealistic lifestyle advice.
- Family education to reduce blame and improve support.
- Referral to a psychologist or psychiatrist when distress is persistent.
- Digital tools or structured self-help as a first step for mild symptoms.
- Better coordination between diabetologists, physicians, dietitians, psychologists, and psychiatrists.
The American Diabetes Association’s Standards of Care are updated annually and include wellbeing and positive health behaviours as part of diabetes care, reflecting the growing recognition that emotional health is not optional in diabetes management.
When should you seek help?
Talk to your doctor if you notice any of the following:
You feel hopeless, guilty, or tired most days.
You avoid checking sugar because it makes you anxious.
You keep sugar high out of fear of hypoglycaemia.
You frequently overeat, restrict, or feel intense shame around food.
You are sleeping poorly for weeks.
You are skipping medicines or appointments because you feel overwhelmed.
You have thoughts of self-harm or death.
The key message
Diabetes care should not stop at HbA1c. A person is not a pancreas, a glucose value, or a prescription chart.
Good diabetes care must ask:
“How is your sugar?”
But also:
“How are you coping?”
“Are you sleeping?”
“Are you scared of lows?”
“Are you tired of managing this?”
“Do you need support?”
Because when the mind is supported, the body becomes easier to care for.
I’ll build this as a longer clinic/website-style article: patient-friendly, but with a stronger research backbone, sections on mechanisms, warning signs, treatment options, and a self-promotion block at the end.
Diabetes is usually measured in numbers: fasting sugar, post-meal sugar, HbA1c, cholesterol, weight, kidney function, blood pressure, and eye check-ups. These numbers matter. But they do not tell the whole story.
A person living with diabetes is not just managing glucose. They are managing food, fear, guilt, family comments, daily medicines, exercise pressure, sleep, work stress, future complications, and sometimes the quiet feeling of being tired of it all.
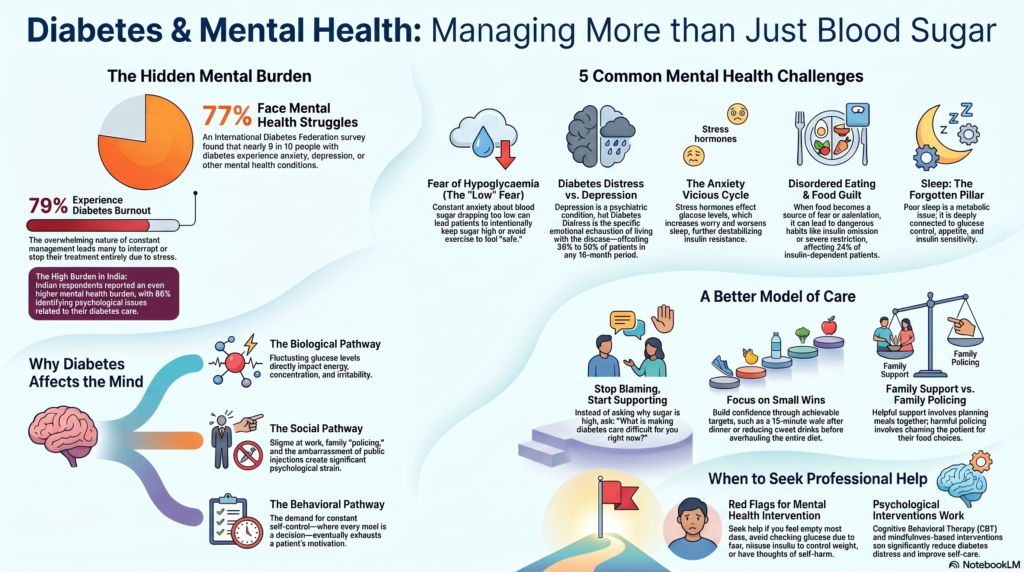
A 2026 review in The Lancet Diabetes & Endocrinology brings this issue into sharp focus. It highlights five common mental health problems in adults living with type 1 diabetes, type 2 diabetes, and gestational diabetes: fear of hypoglycaemia, diabetes distress, depression, disordered eating, and sleep disorders. These are not “minor emotional issues.” They can affect quality of life, self-care, HbA1c, complications, and even premature mortality.
The hidden burden of diabetes
Diabetes care often becomes overly technical. Patients are told to lose weight, walk more, avoid sweets, take medicines, monitor sugar, and come for follow-up. But many are not asked a simple question:
“How are you coping with diabetes emotionally?”
This question matters because diabetes is a 24-hour condition. Unlike an infection that is treated and forgotten, diabetes enters daily life. It enters breakfast, lunch, dinner, travel, festivals, sleep, intimacy, pregnancy planning, work schedules, finances, and family relationships.
The International Diabetes Federation reported in 2024 that 77% of surveyed people living with diabetes had experienced anxiety, depression, or another mental health condition because of diabetes. In the same survey, 79% reported diabetes burnout, and many said they had stopped or interrupted treatment because of stress or feeling overwhelmed. Importantly, Indian respondents reported a particularly high burden, with 86% reporting mental health issues related to diabetes.
This means diabetes care cannot remain limited to sugar control. Good diabetes care must include emotional care.
1. Fear of hypoglycaemia: the fear of sugar going too low
Hypoglycaemia means blood glucose dropping too low. It may cause sweating, tremors, hunger, palpitations, dizziness, confusion, irritability, weakness, or in severe cases, seizures or loss of consciousness.
For people taking insulin or certain oral medicines, this fear can be very real. Some patients begin to live in constant anticipation of a low-sugar episode.
They may think:
“I should eat extra before going out.”
“What if my sugar drops while driving?”
“What if I faint in public?”
“What if it happens at night?”
“Better to keep my sugar slightly high than risk a low.”
This is understandable, but it can become harmful. When fear becomes excessive, people may intentionally keep glucose high, avoid exercise, overeat, reduce medicines without telling the doctor, or check sugar repeatedly in an anxious way.
The solution is not to tell the patient, “Don’t worry.” The solution is to make the diabetes plan safer. This may include reviewing insulin timing, adjusting medications, using continuous glucose monitoring where appropriate, educating the patient and family about hypoglycaemia correction, and treating the anxiety surrounding low sugar.
The CDC also notes that anxiety can sometimes feel like low blood sugar, and low blood sugar can feel like anxiety, making it important to check glucose rather than assume the cause.
2. Diabetes distress: tired of managing diabetes
Diabetes distress is different from depression.
Depression is a psychiatric condition involving persistent low mood, loss of interest, reduced energy, sleep/appetite changes, guilt, hopelessness, and sometimes suicidal thoughts.
Diabetes distress is the emotional exhaustion specifically caused by living with diabetes.
It sounds like:
“I am tired of checking my sugar.”
“I know what I should do, but I cannot keep doing it every day.”
“My family keeps blaming me.”
“Every doctor visit feels like an exam.”
“I feel guilty whenever I eat.”
“I am scared of kidney failure, eye problems, or heart attack.”
“I am doing everything, but my sugar is still high.”
This is one of the most under-recognised problems in diabetes. The CDC notes that diabetes distress may cause people to stop checking blood sugar, slip into unhealthy habits, or skip appointments; it also estimates that in any 18-month period, 33% to 50% of people with diabetes may experience diabetes distress.
A 2025 CDC analysis estimated that about half of US adults with diagnosed diabetes had some level of diabetes distress, showing how common this burden is in real-world populations.
In India, a 2024 systematic review and meta-analysis estimated the pooled prevalence of diabetes distress among people with type 2 diabetes at around 33%, though individual studies varied widely.
The key clinical point is this: diabetes distress is not laziness. It is not lack of discipline. It is emotional overload.
3. Depression and diabetes: a two-way relationship
Depression and diabetes often worsen each other.
When a person is depressed, they may struggle to wake up early, cook healthy food, exercise, attend appointments, check glucose, or take medicines regularly. Depression also increases cravings, sleep disturbance, fatigue, and hopelessness. The CDC notes that depression can interfere with functioning at home and work, including diabetes self-care.
The relationship can also work in the other direction. Diabetes itself can contribute to depression through biological stress, inflammation, lifestyle restriction, fear of complications, sexual dysfunction, neuropathic pain, sleep problems, financial strain, and repeated experiences of failure.
In a clinic, this may appear as “poor compliance.” But beneath poor compliance, there may be untreated depression, diabetes burnout, shame, anxiety, or family conflict.
A patient who is repeatedly missing medicines may not need another lecture. They may need a careful mental health evaluation.
4. Anxiety in diabetes: worry, checking, avoidance
Anxiety in diabetes can take many forms.
Some patients worry constantly about complications. Some become preoccupied with sugar readings. Some panic when glucose fluctuates slightly. Some avoid travel, exercise, driving, or social eating. Some become fearful of injections or blood tests. Others experience health anxiety and repeatedly seek reassurance.
Anxiety can also create a vicious cycle. Stress hormones can affect glucose. High glucose then increases worry. Worry leads to poor sleep. Poor sleep worsens insulin resistance and appetite. Then glucose worsens again.
The CDC states that people with diabetes are 20% more likely than people without diabetes to have anxiety, and that long-term diabetes management can itself be a major source of anxiety.
The goal is not to remove all concern. Some concern is useful. The goal is to convert fear into structured action.
5. Disordered eating: when food becomes fear
Diabetes changes the emotional meaning of food.
A simple meal can become a calculation. Rice, sweets, fruits, snacks, restaurant meals, festivals, and family gatherings may become sources of guilt. Some people become overly restrictive. Some binge after long restriction. Some secretly eat and then feel ashamed. Some avoid social meals. Some become obsessed with weight and glucose numbers.
In insulin-dependent diabetes, disordered eating can become especially dangerous. A 2024 systematic review and meta-analysis found that eating disorder symptoms affected about 24% of people with insulin-dependent diabetes, and insulin omission in adults with insulin-dependent diabetes was estimated at 21%.
This is clinically important because insulin restriction or omission can lead to dangerous hyperglycaemia, diabetic ketoacidosis, and long-term complications.
The message to patients should not be: “You have no control.”
The message should be: “Let us create a food plan that is realistic, flexible, culturally appropriate, and emotionally sustainable.”
For Indian patients, this is especially important because food is not only nutrition. It is family, culture, festivals, hospitality, comfort, and identity. A diabetes plan that ignores this will fail.
6. Sleep disorders: the forgotten pillar of diabetes care
Sleep is often ignored in diabetes consultations. But sleep is deeply connected to glucose control, appetite, weight, energy, mood, and insulin sensitivity.
People with diabetes may sleep poorly because of frequent urination, nocturnal hypoglycaemia, neuropathic pain, restless legs, anxiety, depression, obesity, obstructive sleep apnoea, or irregular work schedules.
A large 2024 retrospective cohort study involving more than one million individuals found that people with newly diagnosed type 2 diabetes had a higher five-year risk of sleep disorders than those without diabetes. The authors concluded that sleep should be regularly discussed as part of holistic diabetes care, especially in younger adults with type 2 diabetes.
Poor sleep is not a lifestyle detail. It is a metabolic and mental health issue.
Why diabetes affects the mind
Diabetes affects mental health through several pathways.
Biological pathway
Fluctuating glucose levels can affect energy, concentration, irritability, and fatigue. Chronic inflammation, insulin resistance, obesity, vascular disease, and hormonal stress systems may also influence mood and cognition.
Behavioural pathway
Diabetes demands repeated self-control. Every meal becomes a decision. Every missed walk can trigger guilt. Every high reading can feel like failure. Over time, this can exhaust motivation.
Social pathway
Many patients face blame from family members: “You ate sweets, that is why this happened.” Some face stigma at work. Some hide insulin use. Some feel embarrassed checking sugar or injecting insulin in public.
Medical pathway
Treatment itself can create psychological strain: injections, fear of hypoglycaemia, weight gain from some medications, cost of medicines, glucose monitoring, and repeated follow-up visits.
Complication pathway
Neuropathy, kidney disease, eye disease, sexual dysfunction, wounds, heart disease, and repeated hospitalisation can all increase depression, anxiety, and hopelessness.
This is why diabetes care must be integrated. The body and mind are not separate departments.
The Indian context: why this matters even more
India has one of the world’s largest diabetes burdens. The ICMR-INDIAB study estimated that in 2021, around 101 million people in India had diabetes and 136 million had prediabetes.
This has major mental health implications. Diabetes in India is often diagnosed in the middle of busy family and work life. Many patients are supporting parents, children, loans, careers, and social obligations. Women may carry additional caregiving burdens. Older adults may have loneliness, cognitive decline, bereavement, and multiple medical illnesses. Younger adults may feel shame or frustration at being diagnosed early.
For many Indian patients, the problem is not lack of advice. The problem is too much advice and too little emotional support.
Patients are told what not to eat, what not to do, and what they are doing wrong. But they are rarely asked what they are finding difficult.
What should doctors screen for?
A good diabetes consultation should include mental health screening when needed. This does not mean every patient needs psychiatric medication. It means emotional burden should be identified early.
Useful areas to screen include:
Depression: persistent sadness, loss of interest, fatigue, hopelessness, guilt, suicidal thoughts.
Anxiety: excessive worry, panic symptoms, fear of complications, fear of hypoglycaemia.
Diabetes distress: feeling overwhelmed by daily diabetes care.
Eating problems: binge eating, severe restriction, guilt around food, insulin omission, weight preoccupation.
Sleep: insomnia, snoring, daytime sleepiness, restless legs, nocturnal hypoglycaemia.
Cognition: memory problems, especially in older adults.
Substance use: alcohol, smoking, or sedative use, which may complicate diabetes care.
The American Diabetes Association’s 2026 Standards of Care updated the psychosocial care section to include behavioural health professionals as integral team members and emphasised screening needs within diabetes care.
What actually helps?
1. Stop blaming the patient
Blame worsens shame. Shame worsens avoidance. Avoidance worsens diabetes.
A better question is:
“What is making diabetes care difficult for you right now?”
2. Make the plan smaller and more practical
Instead of telling someone to change everything, start with two achievable targets.
For example:
Walk 15 minutes after dinner.
Take medicines at the same time daily.
Check sugar twice a week instead of avoiding it completely.
Reduce sweet drinks first before changing the entire diet.
Sleep 30 minutes earlier.
Discuss hypoglycaemia fears with the doctor.
Small wins rebuild confidence.
3. Use psychological interventions
Psychological support can help diabetes distress, depression, anxiety, and self-care. A 2024 systematic review and meta-analysis found that psychological interventions tailored for diabetes distress in adults with type 2 diabetes significantly reduced diabetes distress in the short term, especially when delivered in group formats, by psychologists, with technology components, or among those with elevated baseline distress. However, longer-term effects and HbA1c changes were less clear, meaning follow-up support remains important.
Cognitive behavioural therapy, mindfulness-based interventions, acceptance and commitment therapy, motivational interviewing, problem-solving therapy, family interventions, and structured diabetes education can all be useful depending on the patient.
4. Treat depression and anxiety properly
When depression or anxiety is clinically significant, it should be treated like any other medical condition. Treatment may include psychotherapy, lifestyle restructuring, sleep correction, family intervention, and when needed, medicines.
The choice of antidepressant must consider weight, appetite, sleep, sexual side effects, drug interactions, and the patient’s medical status. This is where coordination between diabetologist, physician, psychiatrist, and psychologist becomes valuable.
5. Address sleep aggressively
Ask about snoring, choking at night, daytime sleepiness, restless legs, late-night screen use, shift work, nocturia, and nighttime hypoglycaemia.
Treating sleep apnoea, insomnia, pain, depression, anxiety, or restless legs may improve both mental health and diabetes self-care.
6. Involve the family, but reduce policing
Family support is useful. Family policing is harmful.
Helpful support sounds like:
“Let us walk together.”
“I will help you plan meals.”
“Let us attend the appointment together.”
“How can I make this easier?”
Unhelpful policing sounds like:
“You caused this.”
“You have no control.”
“You ate rice, now suffer.”
“Your sugar is high because you are careless.”
Diabetes care should be supportive, not punitive.
7. Use digital tools wisely
Digital tools, glucose monitors, reminders, and teleconsultations can help some patients. But they can also worsen anxiety if the person becomes obsessed with every reading.
The goal is informed self-management, not constant self-surveillance.
8. Be careful with new medication narratives
There is growing research on diabetes medications and mental health. For example, a 2026 Lancet Psychiatry study found that GLP-1 receptor agonist use, particularly semaglutide, was associated with lower risk of worsening mental illness among people with diabetes and obesity who already had depression or anxiety. However, this was observational research, so it cannot prove that these medicines directly treat mental illness.
Patients should not start, stop, or change diabetes medicines for mental health reasons without medical supervision.
When should a person with diabetes seek mental health help?
Seek professional help if any of the following are present:
You feel sad, hopeless, guilty, or empty most days.
You have lost interest in things you previously enjoyed.
You feel constantly anxious about sugar readings or complications.
You avoid checking glucose because it scares you.
You intentionally keep sugar high to avoid hypoglycaemia.
You are skipping medicines or appointments because you feel overwhelmed.
You are binge eating, severely restricting, or feeling intense food guilt.
You are misusing insulin or diabetes medicines to control weight.
You are sleeping poorly for weeks.
You are using alcohol, smoking, or sedatives to cope.
You have thoughts of self-harm or death.
Self-harm thoughts require urgent help. This is not something to manage alone.
A better model of diabetes care
The future of diabetes care should not be:
“Your HbA1c is high. Try harder.”
It should be:
“Your HbA1c is high. Let us understand what is making diabetes difficult for you.”
A good diabetes care model should include:
Medical review.
Dietary counselling.
Exercise planning.
Sleep assessment.
Mental health screening.
Family education.
Psychological support.
Medication review.
Relapse prevention.
Long-term follow-up.
This is not “extra care.” This is complete care.
Final message for patients and families
Diabetes is not a character flaw. It is not a punishment. It is not proof that you lack discipline.
It is a chronic medical condition that requires daily decisions. Some days you will manage it well. Some days you will struggle. That does not make you a failure. It makes you human.
The goal is not perfection. The goal is steady, compassionate, practical care.
Your mind matters in diabetes. Your sleep matters. Your fears matter. Your relationship with food matters. Your family environment matters. Your emotional exhaustion matters.
Because when the mind is supported, the body becomes easier to care for.
Need help with diabetes-related stress, depression, anxiety, sleep problems, or emotional eating?
Diabetes care works best when physical health and mental health are addressed together. If you or a loved one is struggling with diabetes distress, fear of low sugar, depression, anxiety, sleep disturbance, emotional eating, or burnout, professional help can make diabetes management more practical and less overwhelming.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery
Opp. Phoenix Mall, Velachery, Chennai
✉ srinivasaiims@gmail.com
📞 +91-8595155808
Related posts:
- Mounjaro (Tirzepatide): A Comprehensive Guide to the Revolutionary Diabetes and Weight Loss Drug
- Ozempic (Semaglutide) – The Breakthrough Weight Loss & Diabetes Drug Taking the World by Storm
- Understanding Geriatric Psychiatry: Why Mental Health Matters in Aging
- Gummies for Mental Health? Why Quick Fixes Can Do More Harm Than Good
- How Acute Inflammation Turns Chronic — And Why It Affects Your Mental Health
- Why Many Indians Abroad Still Return to India for Mental Health Care