Unlocking the Silent Mind: Narcosynthesis Reimagined with Lorazepam
 Introduction
Introduction
There are moments in psychiatry when the mind does not speak.
A patient sits frozen.
A grieving person becomes mute.
A traumatised mind shuts down.
A catatonic patient remains motionless.
A person with dissociation appears present, yet unreachable.
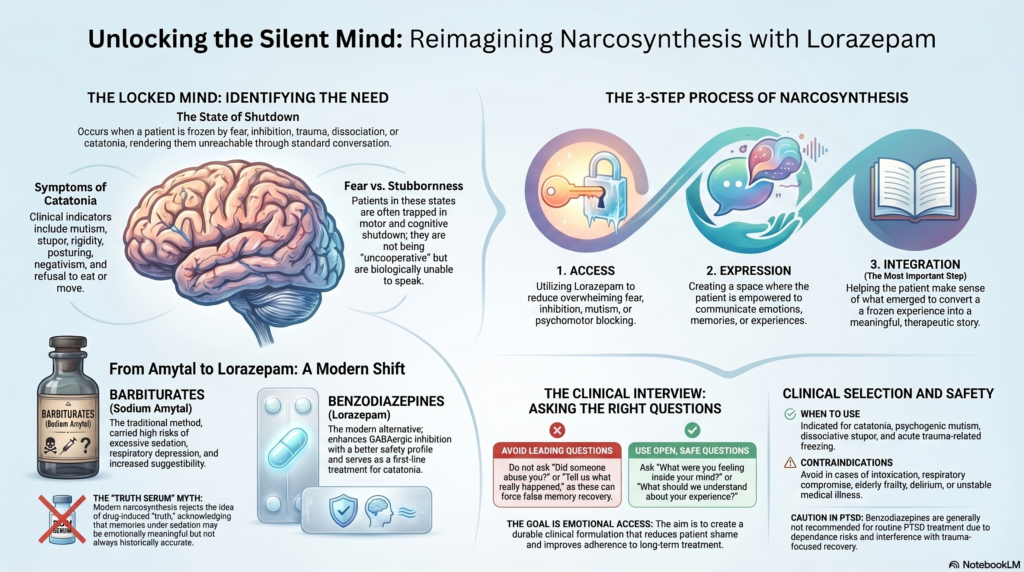
Classical psychiatry had a name for one method of reaching such states: narcosynthesis. Traditionally, it involved the use of sedative drugs such as sodium Amytal to help patients express buried memories, blocked emotions, or traumatic experiences. The older Amytal interview literature emphasised that this method was never a “truth serum”; it had limited usefulness, no diagnostic specificity, and required careful clinical judgement.
Today, sodium Amytal has largely disappeared from routine psychiatric practice. But the core idea remains clinically relevant: sometimes, the problem is not that the patient refuses to speak. The problem is that the mind is locked by fear, inhibition, trauma, dissociation, or catatonia.
In modern psychiatry, lorazepam offers a safer and more familiar way to understand this phenomenon, especially in catatonia and severe anxiety-related shutdown.
What is narcosynthesis?
Narcosynthesis is more than drug-assisted talking.
It involves three steps:
Access: reducing overwhelming fear, inhibition, mutism, or psychomotor blocking.
Expression: allowing the patient to communicate emotions, memories, or experiences.
Integration: helping the patient make sense of what emerged.
This third step is the most important.
Without integration, it is only emotional discharge.
With integration, it becomes therapy.
The goal is not to dig out secrets. The goal is to help the patient convert a frozen experience into a meaningful story.
From Amytal to Lorazepam
Older narcosynthesis used barbiturates such as sodium Amytal. These drugs could reduce inhibition and make patients more communicative, but they carried risks, including excessive sedation, respiratory depression, dependence potential, and increased suggestibility.
Lorazepam belongs to the benzodiazepine group. It enhances GABAergic inhibition and is widely used in psychiatry for acute anxiety, agitation, alcohol withdrawal, seizures, and catatonia. In catatonia, modern guidelines identify benzodiazepines, especially lorazepam, and electroconvulsive therapy as key first-line treatments.
This is where narcosynthesis can be reimagined.
Lorazepam is not used to “recover the truth.” It may create a temporary therapeutic window in which the patient becomes less frozen, less fearful, and more able to communicate.
The silent mind in catatonia
Catatonia is one of the clearest examples of the locked mind.
It may present with:
- mutism,
- stupor,
- staring,
- rigidity,
- posturing,
- negativism,
- refusal to eat,
- immobility,
- agitation,
- echolalia,
- echopraxia.
A patient with catatonia may look uncooperative, but the clinical reality is very different. The person may be trapped in a state of motor, emotional, and cognitive shutdown.
The lorazepam challenge test can produce rapid improvement in some patients with catatonia. A positive response may support the diagnosis and guide treatment, although not all patients respond.
When a mute patient begins to speak after lorazepam, the clinician has a precious opportunity—not to interrogate, but to understand.
The right question is not:
“Now tell us the truth.”
The right question is:
“What were you experiencing when you were unable to speak?”
Lorazepam-assisted synthesis: a modern clinical idea
A modern version of narcosynthesis may be understood as lorazepam-assisted clinical integration.
This means using the temporary improvement created by lorazepam to help the patient and family understand the illness.
For example:
A patient with catatonia receives lorazepam and begins to speak. She says, “I was terrified. I thought if I moved, something terrible would happen.”
This single sentence changes the whole clinical picture.
The family stops seeing her as stubborn.
The clinician understands the fear behind the immobility.
The treatment plan becomes clearer.
The patient feels less ashamed.
That is synthesis.
The medication opens the door.
The therapeutic conversation gives meaning.
Buried memories or blocked emotions?
The phrase “buried memories” is powerful, but it must be used carefully.
Modern psychiatry recognises that memory is not a perfect recording. Under sedation, anxiety relief, or suggestion, patients may produce material that is emotionally meaningful but not always historically accurate.
Therefore, lorazepam-assisted work should avoid leading questions such as:
“Did someone abuse you?”
“Did this happen because of your father?”
“Are you hiding something?”
“Tell us what really happened.”
Instead, the clinician should ask open, safe questions:
“What are you feeling now?”
“What was happening inside your mind?”
“Did you feel afraid?”
“Did you feel stuck?”
“What helped you feel safe?”
“What should we understand about your experience?”
The aim is not forced memory recovery. The aim is safe emotional access.
Where this approach may help
A lorazepam-assisted synthesis approach may be useful in selected cases of:
- catatonia,
- psychogenic mutism,
- severe anxiety shutdown,
- dissociative stupor,
- acute overwhelming grief,
- trauma-related freezing,
- functional neurological symptoms,
- severe panic with inability to communicate.
But it is not suitable for every patient.
It should be avoided or used with extreme caution in:
- intoxication,
- respiratory compromise,
- obstructive sleep apnoea,
- elderly frailty,
- substance dependence,
- delirium,
- severe paranoia,
- unstable medical illness,
- unrealistic expectations of a magical cure.
In trauma and PTSD, benzodiazepines require particular caution. Expert sources generally do not recommend benzodiazepines for PTSD because of limited benefit, dependence risk, and possible interference with trauma-focused recovery.
So, lorazepam-assisted synthesis is not a routine trauma treatment. It is a carefully selected clinical intervention.
The modern psychiatrist’s role
The psychiatrist’s role is not merely to prescribe lorazepam.
The psychiatrist must decide:
Is this catatonia?
Is this dissociation?
Is this psychosis?
Is this severe depression?
Is this trauma shutdown?
Is this functional neurological disorder?
Is there medical illness?
Is the patient safe?
Is the family misunderstanding the condition?
Then comes the key therapeutic task: turning a dramatic response into a durable formulation.
A patient who improves after lorazepam should not leave with the idea, “I was cured by one injection.”
The better explanation is:
“Your brain and body were in a shutdown state. Lorazepam temporarily reduced that block. Now we need to treat the underlying condition and prevent relapse.”
This explanation reduces shame and improves adherence.
Why narcosynthesis still matters
Narcosynthesis reminds us of a timeless truth in psychiatry:
Some symptoms are not merely thoughts.
They are states.
A person can be trapped in fear.
A body can express what the mind cannot say.
A voice can disappear under unbearable affect.
A memory can remain emotionally unprocessed.
A patient can look silent while the mind is screaming.
Modern lorazepam-assisted synthesis is not about truth serum psychiatry. It is about humane psychiatry.
It helps us ask:
What is the patient unable to say?
What is the body trying to communicate?
What fear has frozen the mind?
What story needs careful reconstruction?
What treatment can restore movement, speech, and dignity?
Conclusion
Narcosynthesis reimagined with lorazepam is not a return to outdated truth-serum practices. It is a modern, safer, and more ethical way of understanding selected states where the mind becomes silent.
Lorazepam may temporarily unlock speech, movement, and emotional access—especially in catatonia. But the real healing lies in what follows: careful listening, diagnostic clarity, psychoeducation, psychotherapy, family support, and long-term treatment.
The goal is not to force buried memories into the open.
The goal is to help the silent mind feel safe enough to speak.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808