ICD-11 Personality Disorders: What Has Changed and Why It Matters in Clinical Practice
 There is a quiet discomfort that many clinicians carry, though it is rarely spoken aloud.
There is a quiet discomfort that many clinicians carry, though it is rarely spoken aloud.
We sit with a patient over multiple sessions—sometimes months—and begin to sense a pattern. Not merely symptoms, but a way of being. A recurring rhythm in how the person experiences themselves, relates to others, manages distress, and constructs meaning.
Yet, when the moment comes to diagnose, we are asked to compress this lived complexity into a single word:
Borderline.
Narcissistic.
Avoidant.
The word feels both too much and too little.
Too much—because it risks fixing the person into a rigid identity.
Too little—because it fails to capture the nuance, the movement, the contradictions that define personality.
This tension has long existed at the heart of personality psychiatry.
The older classificatory systems attempted to bring order by dividing personality into types. But in doing so, they often overlooked something essential: personality is not a category—it is a structure, a continuum, and above all, a process unfolding over time.
The ICD-11 represents an attempt to correct this.
Rather than asking, “Which personality disorder does this person have?”
It asks a more clinically honest question:
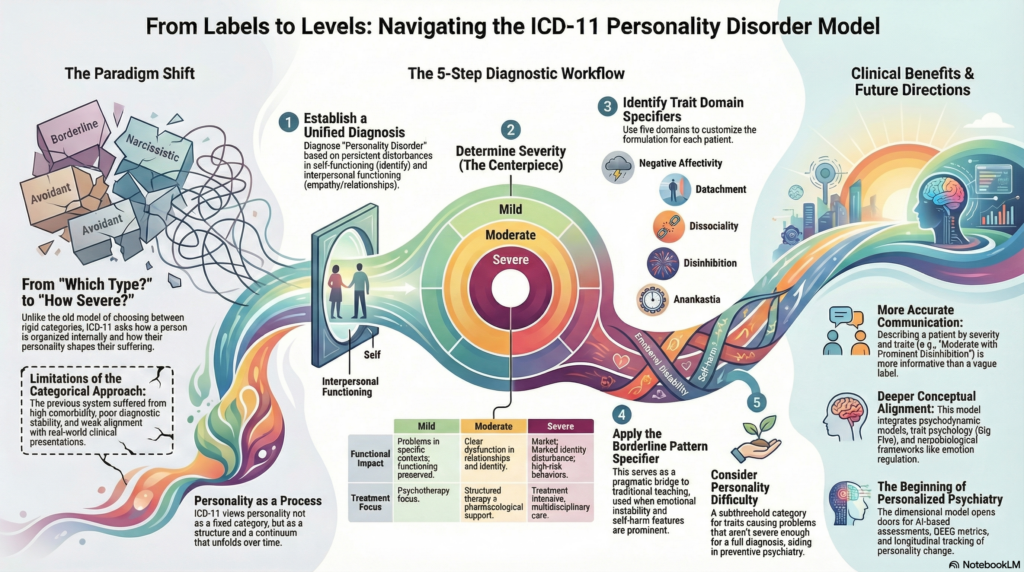
👉 “How is this person organised internally, how impaired are they, and in what ways does their personality shape their suffering?”
This shift—from labels to levels, from categories to configurations—marks a deeper alignment with how clinicians actually understand their patients in practice.
It invites us to move away from naming and toward formulating.
Away from diagnosis as a label, toward diagnosis as a lens into the person’s inner world.
And in doing so, it brings psychiatric classification a step closer to the lived realities of those we treat.
Why ICD-11 Changed the Model
The older systems (ICD-10, DSM-IV/DSM-5 categorical approach) had major limitations:
- High comorbidity (patients met criteria for multiple personality disorders)
- Poor diagnostic stability
- Limited clinical utility
- Weak alignment with real-world presentations
ICD-11 responds to this by focusing on what truly matters clinically:
👉 How severe is the dysfunction?
👉 What kind of personality traits are driving it?
The Core Shift: From Categories to Dimensions
Earlier Approach
- “Does this patient have borderline personality disorder?”
ICD-11 Approach
- “Does this patient have a personality disorder?”
- “How severe is it?”
- “What traits define it?”
This aligns far better with how experienced clinicians actually think.
Step 1: A Single Diagnosis – Personality Disorder
Instead of multiple types, ICD-11 uses:
👉 One unified diagnosis: Personality Disorder
This diagnosis is made when there is:
- Persistent disturbance in:
- Self-functioning (identity, self-direction)
- Interpersonal functioning (relationships, empathy)
- Patterns are:
- Enduring
- Rigid
- Maladaptive across contexts
- Associated with:
- Distress or impairment
Importantly, this is not about “personality traits” alone—
👉 It is about functional impairment driven by personality patterns
Step 2: Severity Becomes the Centerpiece
This is the most important change.
Mild Personality Disorder
- Subtle difficulties
- Problems in specific contexts
- Overall functioning preserved
Moderate Personality Disorder
- Clear dysfunction in relationships and self-identity
- Recurrent interpersonal issues
- Functional impairment across domains
Severe Personality Disorder
- Marked identity disturbance
- Severe relational dysfunction
- High-risk behaviours (self-harm, aggression)
- Significant impairment in most areas of life
👉 Clinically, this is powerful.
Severity predicts:
- Risk
- Prognosis
- Treatment intensity
Step 3: Trait Domain Specifiers
Instead of rigid categories, ICD-11 uses trait domains to describe the personality style.
Negative Affectivity
- Emotional instability, anxiety, vulnerability
Detachment
- Social withdrawal, emotional coldness
Dissociality
- Lack of empathy, disregard for others
Disinhibition
- Impulsivity, poor control
Anankastia
- Perfectionism, rigidity, overcontrol
👉 These traits allow a customised formulation for each patient.
Step 4: Borderline Pattern Specifier
ICD-11 does not discard borderline personality disorder completely.
Instead, it introduces:
👉 “Borderline Pattern” specifier
Used when features include:
- Emotional instability
- Fear of abandonment
- Impulsivity
- Self-harm
This is a pragmatic bridge between traditional teaching and modern classification.
Step 5: Personality Difficulty (Subthreshold Category)
A useful addition:
👉 Personality Difficulty
- Traits causing problems
- But not severe enough for diagnosis
This is particularly valuable in:
- Early identification
- Preventive psychiatry
- Young adults
What This Means for Clinical Practice
1. More Accurate Diagnosis
No more forcing patients into artificial categories.
2. Better Treatment Planning
- Mild → psychotherapy focus
- Moderate → structured therapy + pharmacological support
- Severe → intensive, multidisciplinary care
3. Improved Communication
Describing a patient as:
“Moderate personality disorder with prominent negative affectivity and disinhibition”
…is far more informative than a vague categorical label.
A Deeper Conceptual Insight
ICD-11 aligns closely with:
- Psychodynamic models (identity, relationships)
- Trait psychology (Big Five, dimensional models)
- Neurobiological frameworks (emotion regulation, impulse control)
In essence:
👉 It moves personality disorders from labels → processes
Common Clinical Mistakes (Even Now)
Despite ICD-11, many clinicians still:
- Overuse “borderline” as a catch-all diagnosis
- Ignore severity assessment
- Focus on symptoms rather than personality structure
The ICD-11 model corrects this by forcing a structured, formulation-based approach.
The Future of Personality Psychiatry
This model opens doors for:
- Personalised psychiatry
- Integration with AI-based assessments
- Objective tools (QEEG, CPT, behavioural metrics)
- Longitudinal tracking of personality change
In many ways, ICD-11 is not the endpoint—
👉 It is the beginning of a more data-informed, dimensional psychiatry.
Final Takeaway
ICD-11 asks us to shift from:
❌ “Which personality disorder is this?”
➡️ To
✅ “How severe is the dysfunction, and what traits define it?”
This is a more humane, accurate, and clinically useful way of understanding patients.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
With a clinical approach that integrates:
- Structured ICD-11-based diagnostic frameworks
- Objective assessments (QEEG, CPT)
- AI-assisted clinical synthesis
Dr. Srinivas focuses on accurate diagnosis, personalised treatment, and long-term functional recovery.
If you or your family member are struggling with emotional instability, relationship difficulties, or long-standing behavioural patterns, a comprehensive personality assessment can provide clarity—and a roadmap for change.