CSTC Circuits in Psychiatry
 CSTC stands for:
CSTC stands for:
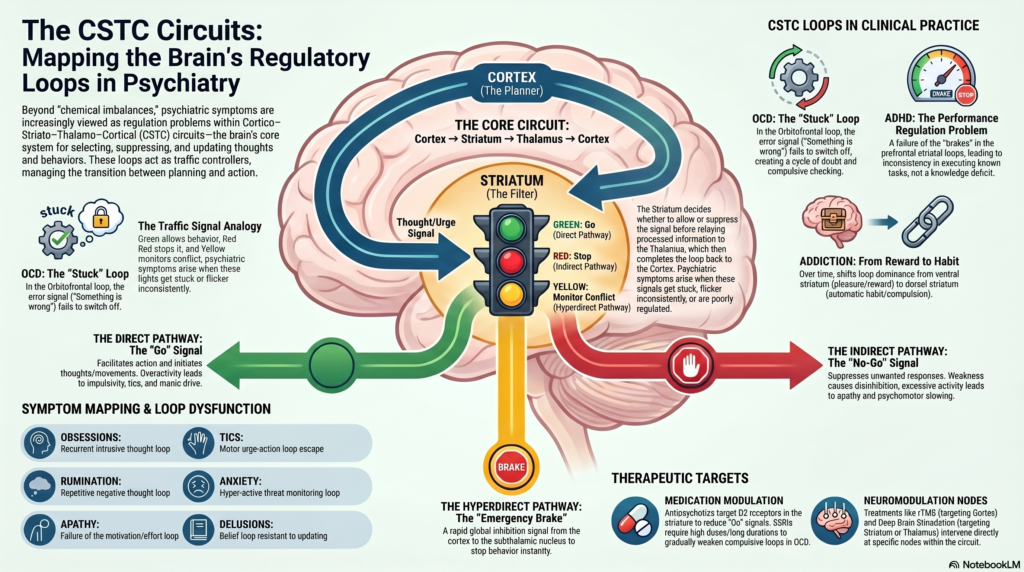
Cortex → Striatum → Thalamus → Cortex
These are repeating brain loops that help regulate:
- Thoughts
- Emotions
- Habits
- Movements
- Motivation
- Compulsions
- Impulses
- Reward-seeking
- Attention
- Behavioural control
In psychiatry, CSTC circuits are important because many symptoms are not just “chemical problems,” but problems of loop regulation.
A useful phrase:
CSTC circuits are the brain’s loop systems for selecting, suppressing, repeating, and updating thoughts and behaviours.
1. Basic CSTC loop
The simplified pathway is:
Cortex → Striatum → Globus Pallidus / Substantia Nigra → Thalamus → Cortex
The cortex sends a plan, urge, thought, or emotional signal to the striatum.
The striatum helps decide whether that signal should be:
- Allowed
- Suppressed
- Repeated
- Strengthened
- Weakened
- Turned into action
The thalamus then sends processed information back to the cortex.
So the system forms a loop.
2. Why loops matter in psychiatry
Many psychiatric symptoms are repetitive loop phenomena.
For example:
| Symptom | Loop problem |
|---|---|
| Obsession | Recurrent intrusive thought loop |
| Compulsion | Repetitive action loop |
| Addiction craving | Reward-seeking loop |
| Tics | Motor urge-action loop |
| Rumination | Repetitive negative thought loop |
| Delusion | Belief loop resistant to updating |
| Anxiety checking | Threat-monitoring loop |
| ADHD impulsivity | Poor inhibition of action loop |
| Catatonia | Motor initiation/inhibition loop disturbance |
So CSTC circuits help psychiatry move from abstract symptom descriptions to brain-based mechanisms.
3. Major CSTC loops
Classically, several parallel CSTC loops are described.
A. Motor loop
Main function:
Movement selection and suppression
Involved regions:
- Motor cortex
- Putamen
- Globus pallidus
- Thalamus
- Motor cortex again
Psychiatric relevance:
- Tics
- Catatonia
- Psychomotor slowing
- Extrapyramidal symptoms
- Antipsychotic-induced parkinsonism
- Tardive dyskinesia
Example:
In tic disorders, the motor loop may permit unwanted motor programs to escape inhibition.
B. Oculomotor loop
Main function:
Eye movement control and visual scanning
Involved regions:
- Frontal eye fields
- Caudate
- Substantia nigra
- Thalamus
- Frontal eye fields
Psychiatric relevance:
- Smooth pursuit abnormalities in schizophrenia
- Eye-tracking deficits
- Attention shifting
- Visual scanning abnormalities
- Possible biomarker research
Example:
In schizophrenia, abnormal eye-tracking may reflect disturbed frontal–striatal coordination.
C. Dorsolateral prefrontal loop
Main function:
Executive function
Involved regions:
- Dorsolateral prefrontal cortex
- Dorsolateral caudate
- Globus pallidus
- Thalamus
- Back to DLPFC
Psychiatric relevance:
- ADHD
- Schizophrenia cognitive symptoms
- Depression-related cognitive slowing
- Executive dysfunction in OCD
- Poor planning
- Poor working memory
Symptoms when impaired:
- Poor concentration
- Poor task completion
- Disorganisation
- Cognitive rigidity
- Poor planning
Example:
A patient knows what to do but cannot sequence, prioritise, and execute the task.
D. Orbitofrontal loop
Main function:
Reward valuation, error detection, emotional decision-making
Involved regions:
- Orbitofrontal cortex
- Ventromedial caudate
- Pallidum
- Thalamus
- Orbitofrontal cortex
Psychiatric relevance:
- OCD
- Addiction
- Impulsivity
- Compulsive checking
- Body dysmorphic disorder
- Eating disorders
- Risky decisions
Symptoms when dysregulated:
- Repeated checking
- Excessive doubt
- Overvaluation of threat
- Compulsive behaviour
- Poor reward-based decision-making
Example:
In OCD, the orbitofrontal loop may keep signalling, “Something is wrong,” even when the situation is safe.
E. Anterior cingulate loop
Main function:
Motivation, effort, conflict monitoring, emotional drive
Involved regions:
- Anterior cingulate cortex
- Ventral striatum
- Pallidum
- Thalamus
- Anterior cingulate cortex
Psychiatric relevance:
- Depression
- apathy
- negative symptoms of schizophrenia
- addiction
- suicidality research
- treatment-resistant depression
- effort-based decision-making
Symptoms when impaired:
- Apathy
- reduced initiative
- emotional pain
- poor effort mobilisation
- indecision
- low drive
Example:
A patient may want recovery but cannot mobilise effort into action.
F. Limbic / ventral striatal loop
Main function:
Reward, pleasure, craving, emotional learning
Involved regions:
- Ventromedial prefrontal cortex
- Amygdala
- Hippocampus
- Nucleus accumbens
- Ventral pallidum
- Mediodorsal thalamus
- Prefrontal cortex
Psychiatric relevance:
- Addiction
- depression
- mania
- psychosis
- reward sensitivity
- anhedonia
- craving
- emotional dysregulation
Example:
In addiction, the ventral striatal loop assigns excessive motivational value to drug cues.
4. Direct and indirect pathways
The CSTC system has two important functional pathways.
Direct pathway: “Go” pathway
The direct pathway facilitates action.
It says:
“Allow this behaviour.”
It helps initiate selected thoughts, behaviours, movements, or responses.
Too much direct pathway activity may contribute to:
- impulsivity
- tics
- compulsions
- manic drive
- addiction-seeking behaviour
Indirect pathway: “No-Go” pathway
The indirect pathway suppresses action.
It says:
“Stop this behaviour.”
It helps inhibit unwanted responses.
Weak indirect pathway control may contribute to:
- disinhibition
- impulsivity
- compulsions
- tics
- poor behavioural control
Excessive inhibition may contribute to:
- psychomotor slowing
- apathy
- catatonia-like states
- Parkinsonian features
5. Hyperdirect pathway
There is also a rapid stopping pathway:
Cortex → Subthalamic nucleus → Globus pallidus → Thalamus
This is called the hyperdirect pathway.
It helps with fast global inhibition.
It is like an emergency brake.
Psychiatric relevance:
- impulsivity
- OCD
- stopping behaviour
- impulse control disorders
- deep brain stimulation targets
Example:
In impulsivity, the emergency brake may not activate quickly enough.
6. CSTC and OCD
OCD is one of the clearest CSTC disorders.
Commonly implicated loop:
Orbitofrontal cortex → caudate → thalamus → orbitofrontal cortex
The problem:
- Error signal remains active
- Threat signal does not switch off
- Doubt persists
- Compulsion temporarily reduces anxiety
- Loop strengthens over time
Clinical example:
“I know the door is locked, but it doesn’t feel locked.”
This is not just memory failure. It is a loop problem involving error detection, doubt, threat valuation, and compulsive action.
OCD loop summary
| Component | Clinical expression |
|---|---|
| Orbitofrontal cortex | “Something is wrong” |
| Anterior cingulate | Anxiety and conflict |
| Caudate | Failure to filter repetitive signal |
| Thalamus | Sends signal back to cortex |
| Compulsion | Temporarily reduces distress but reinforces loop |
7. CSTC and ADHD
In ADHD, CSTC circuits involving the prefrontal cortex, striatum, and thalamus are relevant to:
- attention
- inhibition
- working memory
- reward sensitivity
- delay aversion
- motivation
Affected loops:
- DLPFC loop
- anterior cingulate loop
- frontostriatal reward loop
Clinical expression:
- difficulty sustaining attention
- impulsive responses
- poor working memory
- preference for immediate reward
- difficulty delaying gratification
- inconsistency in performance
A useful ADHD phrase:
ADHD is not a knowledge deficit; it is a performance regulation problem.
CSTC circuits help explain why a person may know what to do but cannot reliably do it at the right time.
8. CSTC and addiction
Addiction strongly involves the ventral striatal CSTC loop.
Important regions:
- Prefrontal cortex
- nucleus accumbens
- amygdala
- hippocampus
- thalamus
- dopamine pathways
Clinical process:
- Drug produces reward
- Brain learns cue-reward association
- Cues trigger craving
- Prefrontal control weakens
- Habit circuits take over
- Use continues despite harm
Over time, addiction shifts from:
Reward-seeking → habit-driven compulsion
This involves transition from ventral striatum to dorsal striatum.
Clinical example:
The patient may no longer use only for pleasure. They use to feel normal, avoid withdrawal, or obey a learned habit loop.
9. CSTC and schizophrenia
In schizophrenia, CSTC dysfunction may contribute to:
- abnormal salience
- impaired belief updating
- cognitive symptoms
- negative symptoms
- motor abnormalities
- catatonia
- psychosis-related certainty
Striatal dopamine dysregulation is central to psychosis. But CSTC loops explain how abnormal dopamine can affect beliefs, action selection, and salience.
Clinical example:
A neutral event receives excessive salience, enters a belief loop, and becomes difficult to update despite contrary evidence.
This may contribute to delusional conviction.
10. CSTC and depression
Depression involves CSTC-related disturbances in:
- reward processing
- motivation
- psychomotor speed
- cognitive control
- emotional regulation
Relevant loops:
- anterior cingulate loop
- ventral striatal loop
- DLPFC loop
Clinical expression:
- anhedonia
- apathy
- indecision
- psychomotor slowing
- rumination
- poor cognitive control over negative thoughts
Example:
The patient may not merely feel sad; the brain’s motivation and reward loops fail to generate energy toward action.
11. CSTC and bipolar disorder
In bipolar disorder, CSTC circuits may be involved in:
- reward hypersensitivity
- impulsivity
- goal-directed overactivity
- risk-taking
- reduced inhibition
- manic drive
During mania, the “go” systems may dominate over inhibitory control.
Clinical expression:
- excessive plans
- overspending
- increased sexuality
- decreased sleep
- rapid decisions
- grandiose goal pursuit
In depression, the same broader circuits may shift toward reduced reward and low drive.
12. CSTC and tic disorders
Tics are strongly related to basal ganglia and CSTC circuits.
The motor loop may fail to suppress unwanted motor or vocal programs.
Clinical expression:
- motor tics
- vocal tics
- premonitory urges
- temporary relief after tic
- worsening with stress
- partial voluntary suppression
Example:
The patient feels an urge rising, performs the tic, and experiences brief relief.
This resembles a motor-compulsive loop.
13. CSTC and catatonia
Catatonia may involve disturbance in motor, limbic, and frontal-basal ganglia circuits.
Clinical expression:
- stupor
- mutism
- posturing
- negativism
- rigidity
- excitement
- stereotypy
CSTC circuits may help explain why motor initiation and inhibition become profoundly disturbed.
This is also why GABAergic treatment with benzodiazepines can be effective in many cases.
14. CSTC and anxiety
Anxiety involves threat detection and safety behaviour loops.
Relevant circuits:
- amygdala
- prefrontal cortex
- striatum
- thalamus
- anterior cingulate
Clinical expression:
- checking
- avoidance
- reassurance seeking
- hypervigilance
- safety behaviours
Example:
Avoidance reduces anxiety temporarily but reinforces the loop long-term.
This is similar to compulsive reinforcement.
15. CSTC and eating disorders
CSTC circuits may contribute to:
- habit formation
- body checking
- compulsive exercise
- rigid food rules
- reward alteration
- cognitive inflexibility
In anorexia nervosa, there may be excessive cognitive control, habit rigidity, and altered reward processing.
In binge eating, reward and impulse-control loops may be more prominent.
16. CSTC and personality disorders
CSTC circuits are not “personality disorder circuits,” but they can help explain dimensions such as:
- impulsivity
- emotional dysregulation
- reward sensitivity
- aggression
- habit loops
- self-harm urges
- compulsive relational patterns
For example, in borderline personality disorder:
- limbic salience may be high
- prefrontal inhibition may be unstable
- reward/threat loops may shift rapidly
- interpersonal cues may become strongly salient
This can produce fast emotional-action loops.
17. Neurotransmitters in CSTC circuits
Several neurotransmitters shape CSTC function.
| Neurotransmitter | CSTC role |
|---|---|
| Dopamine | Reward, salience, action selection |
| Glutamate | Cortical input, learning, plasticity |
| GABA | Inhibition, filtering, rhythm |
| Serotonin | Impulse control, mood regulation |
| Acetylcholine | Attention, striatal modulation |
| Noradrenaline | arousal, vigilance, effort |
This is why different medications affect different aspects of CSTC functioning.
18. Medication relevance
Antipsychotics
Antipsychotics reduce dopamine signalling, especially D2-mediated striatal activity.
Benefits:
- reduce psychosis
- reduce mania
- reduce agitation
- reduce tics in some cases
Adverse effects from CSTC perspective:
- parkinsonism
- akathisia
- dystonia
- emotional blunting
- tardive dyskinesia
These side effects occur because dopamine blockade also affects motor CSTC loops.
SSRIs
SSRIs are useful in OCD and anxiety partly because they modulate cortico-striatal loops over time.
In OCD, improvement usually takes:
- higher dose
- longer duration
- sustained treatment
This fits the idea that compulsive loops take time to weaken.
Stimulants and atomoxetine
In ADHD, stimulants and noradrenergic agents improve signal-to-noise in frontostriatal circuits.
They can improve:
- attention
- inhibition
- task persistence
- working memory
- motivation
Benzodiazepines
In catatonia, benzodiazepines may restore inhibitory balance through GABA-A mechanisms.
This can rapidly improve motor and behavioural symptoms in responsive cases.
19. Neuromodulation relevance
CSTC circuits are highly relevant to neuromodulation.
rTMS
Targets cortical nodes, such as:
- DLPFC in depression
- supplementary motor area in tics/OCD research
- temporoparietal cortex in hallucinations
DBS
Deep brain stimulation targets CSTC-related structures in severe refractory illness.
Examples:
- OCD: anterior limb of internal capsule, nucleus accumbens, subthalamic nucleus
- Depression: subcallosal cingulate, ventral capsule/ventral striatum
- Tourette syndrome: thalamic and basal ganglia targets
Neurofeedback
May aim to improve self-regulation of attention, arousal, and cortical control, indirectly influencing CSTC dynamics.
Summary
CSTC circuits are the brain’s repeating loops for selecting, inhibiting, and reinforcing thoughts and behaviours; when these loops become overactive, underactive, or poorly regulated, psychiatric symptoms emerge.
Think of CSTC circuits as a traffic signal system.
- Green signal = allow behaviour
- Red signal = stop behaviour
- Yellow signal = monitor conflict
- Faulty signal = repetitive, impulsive, stuck, or inhibited behaviour
In OCD, the red/yellow warning signal does not switch off.
In ADHD, the brake signal is inconsistent.
In addiction, the reward route becomes overlearned.
In schizophrenia, salience and belief loops become unstable.
In depression, motivation loops slow down.
In mania, goal-directed drive becomes excessive.
CSTC circuits are central to modern psychiatry because they explain how symptoms become repetitive, compulsive, impulsive, motivational, cognitive, or motoric.
They help connect:
- OCD compulsions
- ADHD impulsivity
- addiction craving
- schizophrenia delusions
- depression apathy
- mania overactivity
- tics
- catatonia
- antipsychotic motor side effects
Psychiatry is not only about neurotransmitters. It is also about loops.
CSTC circuits are some of the most important loops in the brain.