Abdominal Migraine: A Gut–Brain Disorder with Important Psychiatric Dimensions
 Introduction
Introduction
Abdominal migraine is an under-recognised migraine-related disorder in which the main symptom is recurrent abdominal pain, rather than headache. It is classically described in children, but adult presentations are increasingly being reported. The condition is often mistaken for gastritis, irritable bowel syndrome, food intolerance, recurrent “stomach infection,” or stress-related abdominal pain.
The typical pattern is distinctive: repeated episodes of central or periumbilical abdominal pain, often associated with nausea, vomiting, pallor, loss of appetite, light sensitivity or headache, with the person returning to normal health between attacks. A recent adult case report described a 47-year-old woman with recurrent abdominal pain and vomiting, normal investigations, a childhood history of migraine, and improvement with sumatriptan, supporting the view that abdominal migraine may be overlooked in adults.
What is abdominal migraine?
Abdominal migraine is best understood as an episodic disorder of the gut–brain axis. The abdominal pain is usually severe enough to interfere with routine activities. Attacks may last for hours and recur in a stereotyped pattern. Between episodes, the person is usually well.
Common associated symptoms include:
| Symptom cluster | Clinical features |
|---|---|
| Gastrointestinal | Central abdominal pain, nausea, vomiting, anorexia |
| Migraine-like | Headache, photophobia, phonophobia, pallor |
| Autonomic | Sweating, fatigue, dizziness, lethargy |
| Functional impact | School absence, work disruption, emergency visits, avoidance of travel or food |
A strong personal or family history of migraine increases clinical suspicion. In children, abdominal migraine may later evolve into typical migraine headache. In adults, the diagnosis is often delayed because clinicians may not immediately connect recurrent abdominal pain with migraine biology.
Why abdominal migraine is often missed
Abdominal migraine is frequently missed because abdominal pain naturally leads patients first to gastroenterology, not neurology or psychiatry. Repeated blood tests, scans, endoscopy and ultrasound may be normal. When investigations are unrevealing, patients may be told that the pain is “just stress” or “functional,” which can feel dismissive.
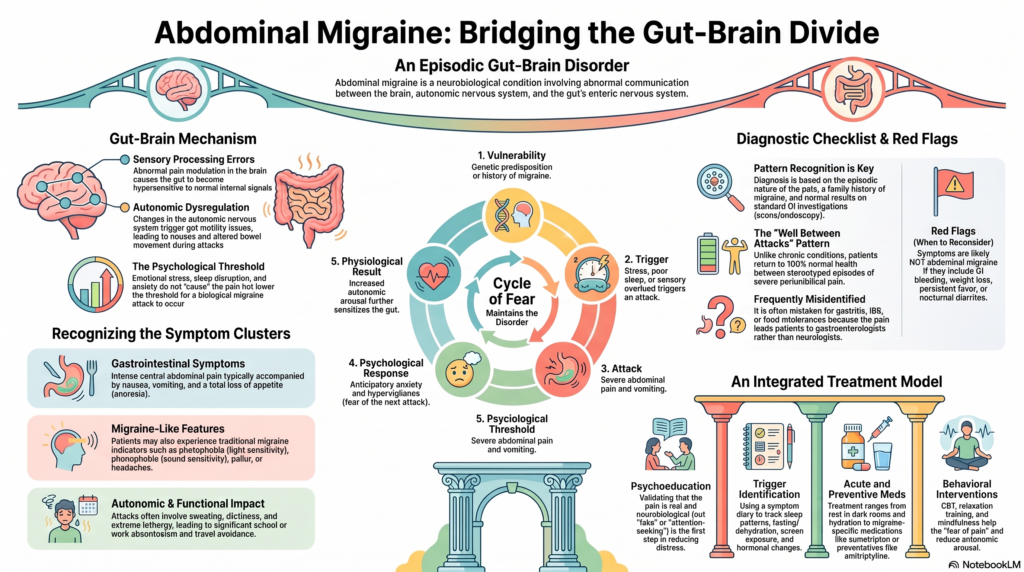
The correct framing is different: abdominal migraine is not imaginary. It is a real neurobiological condition involving abnormal communication between the brain, autonomic nervous system, enteric nervous system, pain pathways and gastrointestinal motility.
Abdominal migraine overlaps with other gut–brain disorders such as cyclic vomiting syndrome, and that both conditions may share migraine-related mechanisms.
The gut–brain axis: the central concept
The gut has its own complex nervous system, called the enteric nervous system, which communicates continuously with the brain through neural, hormonal, immune and autonomic pathways. In abdominal migraine, this gut–brain communication may become dysregulated.
Several mechanisms may contribute:
| Mechanism | Possible role |
|---|---|
| Migraine biology | Abnormal sensory processing and pain modulation |
| Autonomic dysregulation | Nausea, pallor, sweating, dizziness and gut motility changes |
| Visceral hypersensitivity | The gut becomes more sensitive to normal internal signals |
| Gastric dysmotility | Delayed or altered gut movement during attacks |
| Stress-response activation | Emotional stress lowers the threshold for attacks |
| Genetic vulnerability | Family history of migraine is common |
This is where psychiatric understanding becomes clinically important.
Psychiatric aspects of abdominal migraine
Psychiatric factors do not mean the pain is “psychological” or “not real.” Instead, they help explain why the gut and brain can amplify each other.
Abdominal migraine often exists at the intersection of neurology, gastroenterology and psychiatry. Anxiety, sleep disruption, emotional stress, sensory sensitivity and autonomic arousal can all lower the threshold for attacks. Once attacks become recurrent, the patient may develop anticipatory anxiety: fear of the next episode, fear of vomiting in public, fear of eating certain foods, fear of travel, school avoidance or work avoidance.
This creates a cycle:
migraine vulnerability → abdominal attack → fear and hypervigilance → autonomic arousal → gut sensitivity → more attacks
In children, this may present as school refusal, repeated visits to the sick room, separation anxiety, irritability or reduced participation in sports and social activities. In adults, it may appear as health anxiety, repeated emergency consultations, dietary restriction, work absenteeism, panic-like symptoms or avoidance of travel and meetings.
Important psychiatric comorbidities
A careful psychiatric assessment should look for:
| Comorbidity | Why it matters |
|---|---|
| Anxiety disorders | Increase anticipatory fear, autonomic arousal and symptom monitoring |
| Panic disorder | Can mimic or amplify nausea, abdominal discomfort and dizziness |
| Depression | Worsens pain perception, sleep, appetite and functioning |
| Somatic symptom disorder | May coexist when health anxiety and preoccupation become excessive |
| Trauma-related symptoms | Can increase bodily threat perception and autonomic reactivity |
| Eating disorders | Must be considered when vomiting, food avoidance or weight loss is present |
| Sleep disorders | Poor sleep is a major migraine trigger |
| Substance use | Cannabis hyperemesis syndrome must be ruled out in recurrent vomiting |
The goal is not to label the patient as “psychiatric.” The goal is to create a complete biopsychosocial formulation.
Diagnostic approach
Abdominal migraine is a diagnosis of pattern recognition plus exclusion of serious medical causes. The clinician should ask:
- Is the pain episodic and stereotyped?
- Is the person well between attacks?
- Are there migraine-like features such as nausea, vomiting, pallor, headache or light sensitivity?
- Is there a personal or family history of migraine?
- Are investigations normal or not suggestive of another disorder?
- Are there psychological or sleep-related triggers?
- Is there functional impairment at school, work or home?
The diagnosis should be reconsidered if symptoms are continuous, progressively worsening, localised to one fixed area, associated with gastrointestinal bleeding, persistent fever, weight loss, anaemia, abnormal inflammatory markers, nocturnal diarrhoea, delayed growth in children, neurological deficits or new-onset severe symptoms in older adults.
Differential diagnosis
Abdominal migraine can resemble several conditions:
| Condition | Key distinction |
|---|---|
| Gastritis/peptic disease | More meal-related, burning pain, endoscopic findings may be present |
| IBS | More bowel habit change; pain often linked to stooling |
| Cyclic vomiting syndrome | Vomiting is the dominant feature |
| Biliary disease | Right upper quadrant pain, food relation, ultrasound/HIDA abnormalities |
| Pancreatitis | Elevated enzymes, persistent severe pain |
| Food intolerance | Clear dietary relationship |
| Panic attacks | Prominent fear, palpitations, breathlessness and acute anxiety |
| Somatic symptom disorder | Excessive health preoccupation may dominate the clinical picture |
| Cannabis hyperemesis | Cannabis use, relief with hot showers, recurrent vomiting |
Treatment: an integrated model
Management is most effective when medical and psychological approaches are combined.
1. Psychoeducation
Patients and families need a clear explanation: abdominal migraine is a real gut–brain disorder. It is not “fake,” not “attention-seeking,” and not merely “gas.” This validation itself reduces distress and unnecessary investigations.
2. Trigger identification
A symptom diary can track:
| Trigger domain | Examples |
|---|---|
| Sleep | Late nights, irregular sleep, sleep deprivation |
| Food pattern | Fasting, dehydration, skipped meals |
| Sensory | Bright light, noise, screen exposure |
| Emotional | Exams, work stress, conflict, separation anxiety |
| Hormonal | Menstrual association |
| Physical | Travel, exertion, exhaustion |
3. Acute attack plan
During an attack, the patient may benefit from rest in a quiet dark room, hydration, antiemetics, simple analgesics when appropriate, and migraine-specific abortive treatment in selected cases. Some studies report improvement with sumatriptan, though not all patients respond similarly.
4. Preventive medication
For frequent or disabling attacks, migraine-preventive medicines may be considered. Options described in the literature include beta-blockers, calcium-channel blockers, topiramate, valproate, amitriptyline and cyproheptadine. Choice depends on age, comorbidities, adverse-effect profile and specialist evaluation.
5. Psychiatric and behavioural interventions
Psychiatric care can reduce attack frequency, disability and fear around symptoms. Useful interventions include:
| Intervention | Clinical benefit |
|---|---|
| CBT for pain | Reduces catastrophising, avoidance and symptom fear |
| Relaxation training | Reduces autonomic arousal |
| Breathing techniques | Helps nausea, panic-like sensations and bodily tension |
| Mindfulness | Improves tolerance of bodily sensations |
| Biofeedback | Helps autonomic regulation in selected patients |
| Sleep therapy | Reduces migraine threshold |
| Family intervention | Prevents overprotection and reinforces normal routine |
| Treatment of anxiety/depression | Improves pain coping and overall functioning |
In children, the aim is to support gradual return to school and activity. In adults, the aim is to restore confidence in eating, travel, work and daily functioning.
The psychiatrist’s role
A psychiatrist can help in several ways:
- Identify anxiety, depression, panic symptoms, trauma-related factors or health anxiety.
- Explain the gut–brain model in a non-stigmatising way.
- Reduce avoidance behaviours that maintain disability.
- Improve sleep and stress regulation.
- Use CBT-based strategies for pain coping.
- Coordinate care with gastroenterology, neurology and paediatrics.
- Choose medications carefully when migraine prevention and psychiatric symptoms overlap.
Amitriptyline, for example, may be useful in some patients because it can target migraine prevention, visceral pain sensitivity, sleep and anxiety symptoms. However, it must be individualised and monitored for side effects.
Key message
Abdominal migraine is a real and often under-recognised gut–brain disorder. It should be suspected when abdominal pain is recurrent, stereotyped, disabling, associated with nausea, vomiting, pallor or migraine features, and followed by complete wellness between attacks.
Psychiatric aspects are central to understanding abdominal migraine, but they should never be used to dismiss the patient’s suffering. Anxiety, stress, sleep disturbance and autonomic arousal can trigger or amplify attacks, while repeated attacks can create fear, avoidance and disability. The best outcomes come from an integrated approach: accurate diagnosis, migraine-oriented treatment, trigger control, sleep correction, psychiatric assessment, behavioural therapy and restoration of normal functioning.
About the Author
Dr. Srinivas Rajkumar T
MD Psychiatry, AIIMS New Delhi
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808