Role of a Psychiatrist in Stroke Management: Mind, Mood, Behaviour and Recovery
 Stroke is usually understood as a neurological emergency affecting movement, speech, swallowing, vision or balance. But recovery after stroke is not only physical. A stroke can also affect mood, motivation, sleep, cognition, personality, emotional control, behaviour, family relationships and rehabilitation participation.
Stroke is usually understood as a neurological emergency affecting movement, speech, swallowing, vision or balance. But recovery after stroke is not only physical. A stroke can also affect mood, motivation, sleep, cognition, personality, emotional control, behaviour, family relationships and rehabilitation participation.
This is where the psychiatrist has an important role.
A psychiatrist does not replace the neurologist, physician or rehabilitation team. Instead, the psychiatrist works alongside them to identify and treat the neuropsychiatric consequences of stroke — especially post-stroke depression, anxiety, emotionalism, apathy, cognitive impairment, psychosis, delirium, sleep problems and caregiver distress.
In simple terms, the psychiatrist asks:
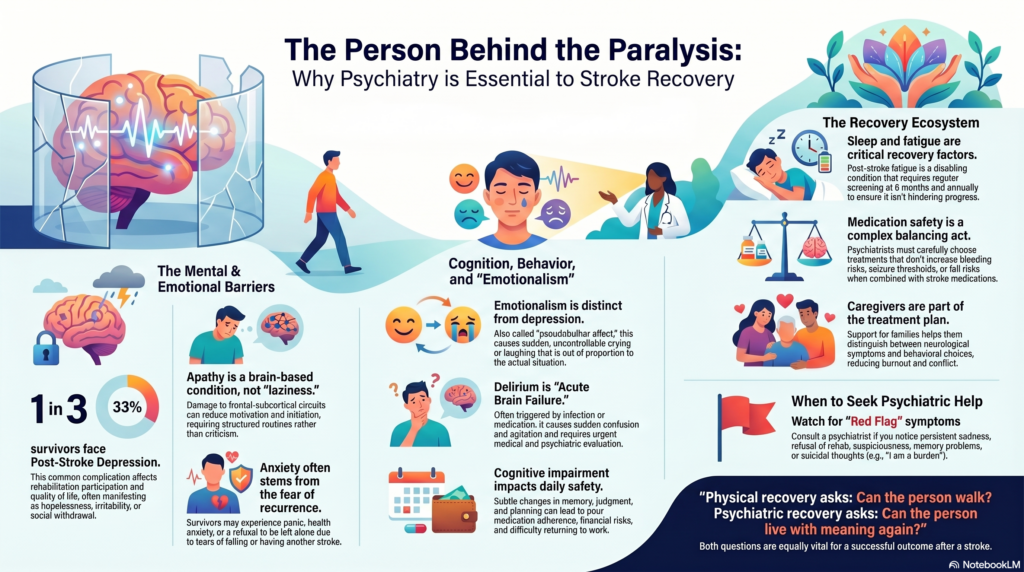
“What is happening to the person behind the paralysis?”
Stroke recovery is not only physical recovery
Modern stroke rehabilitation guidelines emphasise that people after stroke need assessment for multiple common post-stroke problems, including communication, cognition, fatigue, mood, safety, function and participation. NICE’s 2023 stroke rehabilitation guideline states that rehabilitation should ensure people are assessed for common stroke-linked problems and receive the care and therapy they need in hospital and the community.
This matters because a patient may regain limb strength but still struggle with:
depression, anxiety, irritability, loss of confidence, poor sleep, emotional outbursts, memory problems, impulsivity, reduced motivation, fatigue, personality change or caregiver conflict.
If these are missed, physical rehabilitation also suffers.
1. Diagnosing and treating post-stroke depression
Post-stroke depression is one of the most common and important psychiatric complications after stroke. It can occur soon after stroke or months later, and it may significantly affect rehabilitation, quality of life, functional recovery and caregiver burden.
The American Heart Association/American Stroke Association scientific statement describes post-stroke depression as common and reports that it affects about one-third of stroke survivors at any one time after stroke.
Post-stroke depression may present as:
low mood, crying spells, hopelessness, reduced interest, poor sleep, loss of appetite, fatigue, irritability, social withdrawal, poor therapy participation, thoughts of being a burden, or suicidal ideas.
A psychiatrist helps distinguish depression from:
normal grief after disability,
fatigue,
aphasia-related frustration,
cognitive impairment,
apathy,
medication effects,
or neurological slowing.
Treatment may include psychoeducation, supportive psychotherapy, behavioural activation, family counselling, structured rehabilitation goals and antidepressants when clinically indicated.
2. Managing post-stroke anxiety and fear
Many stroke survivors become anxious after the event. They may fear another stroke, fear falling, fear being alone, fear losing independence, or fear returning to work.
Anxiety may appear as:
persistent worry, panic-like episodes, sleep disturbance, health anxiety, avoidance of walking, refusal to be left alone, irritability, repeated checking of blood pressure, or excessive reassurance-seeking.
A psychiatrist helps assess whether anxiety is related to:
fear of recurrence,
loss of confidence,
post-stroke trauma,
motor disability,
speech difficulty,
cardiac symptoms,
medication effects,
or co-existing depression.
Canadian Stroke Best Practice material recommends that people with stroke who have one mood disorder, such as depression, should be assessed for others, such as anxiety. It also highlights psychological interventions such as motivational interviewing or problem-solving therapy before considering antidepressant medication in suitable cases.
3. Understanding apathy after stroke
Apathy after stroke is often mistaken for laziness or lack of cooperation.
Families may say:
“He is not trying.”
“She has given up.”
“He does not participate in physiotherapy.”
“She just sits silently.”
But apathy can be a brain-based reduction in motivation and initiation, especially after frontal-subcortical circuit involvement. It may occur with depression, but it can also occur without sadness.
A psychiatrist helps differentiate:
apathy from depression,
fatigue from low motivation,
cognitive impairment from disinterest,
aphasia from withdrawal.
Management includes structured routines, external cueing, short achievable goals, pleasant activity scheduling, caregiver education, sleep correction, treatment of depression if present, and close coordination with the rehabilitation team.
This reframing is often therapeutic for the family. The patient is not “lazy.” The stroke may have affected the brain systems that initiate action.
4. Managing emotionalism and emotional lability
Some stroke survivors cry or laugh suddenly, excessively or in a way that feels out of proportion to the situation. Families may misinterpret this as severe depression, attention-seeking or loss of control.
This can be due to post-stroke emotionalism, also called emotional lability or pseudobulbar affect.
The psychiatrist helps identify whether the crying is due to:
depression,
grief,
frustration,
emotionalism,
fatigue,
or communication difficulty.
This distinction matters because emotionalism and depression are related but not identical. The treatment approach may include psychoeducation, reassurance, family training and medication in selected cases.
5. Assessing cognition after stroke
Stroke can affect attention, memory, processing speed, planning, judgement, language, visuospatial ability and executive functioning.
Post-stroke cognitive impairment may show up as:
forgetfulness, poor planning, impulsive decisions, difficulty managing money, inability to follow rehabilitation instructions, poor medication adherence, getting lost, reduced safety awareness, or difficulty returning to work.
A psychiatrist helps distinguish:
post-stroke cognitive impairment,
vascular cognitive impairment,
vascular dementia,
delirium,
depression-related cognitive impairment,
aphasia-related testing difficulty,
and medication-induced cognitive dulling.
NICE stroke rehabilitation guidance emphasises goal-setting, accessible information and support for the person after stroke to participate actively in decisions. This is particularly important when cognition, communication or insight is affected.
The psychiatrist can also help the family plan supervision, financial safety, driving decisions, work fitness and long-term cognitive monitoring.
6. Identifying delirium and acute confusion
A stroke patient who suddenly becomes confused, agitated, drowsy, suspicious or hallucinating may have delirium.
This is especially common in older adults, patients with infection, dehydration, sleep deprivation, metabolic disturbance, polypharmacy or prolonged hospital stay.
Delirium is not “madness.” It is an acute brain failure state and often signals a medical problem.
The psychiatrist’s role is to:
identify delirium early,
review precipitating factors,
avoid unnecessary sedatives,
recommend safer behavioural strategies,
coordinate medical evaluation,
and guide short-term medication only when needed for safety.
This is particularly important because excessive sedation can worsen swallowing, falls, aspiration risk, cognition and rehabilitation participation.
7. Managing post-stroke psychosis, suspiciousness and behaviour change
Less commonly, stroke may be followed by hallucinations, delusions, suspiciousness, personality change, disinhibition or aggression.
This may occur due to:
stroke location,
delirium,
post-stroke dementia,
sleep deprivation,
medication effects,
sensory impairment,
depression with psychotic symptoms,
or pre-existing psychiatric vulnerability.
The psychiatrist helps determine the cause and decide whether medication is required. In older stroke survivors, antipsychotics must be used carefully because of sedation, falls, stroke risk, metabolic effects and cognitive worsening.
The goal is not to suppress the patient, but to reduce distress and risk while preserving function.
8. Helping with sleep and fatigue
Sleep problems and fatigue are very common after stroke. Patients may have insomnia, fragmented sleep, daytime sleepiness, obstructive sleep apnoea, restless legs, pain-related sleep disruption, anxiety-related insomnia or depression-related early morning waking.
Post-stroke fatigue can be disabling. It is not simply tiredness.
The 2023 National Clinical Guideline for Stroke recommends periodic review for post-stroke fatigue and assessment of factors that may precipitate or worsen fatigue, including depression, anxiety, sleep disorders and pain. It recommends review at discharge and then at regular intervals, including 6 months and annually thereafter.
A psychiatrist helps by assessing whether fatigue is related to:
depression, anxiety, poor sleep, pain, medication, cognitive overload, emotional distress, or unrealistic rehabilitation pacing.
Better sleep and fatigue management can improve therapy participation and family functioning.
9. Supporting rehabilitation adherence
Psychiatric symptoms directly affect rehabilitation outcomes.
A depressed patient may not participate.
An anxious patient may avoid walking.
An apathetic patient may not initiate exercises.
A cognitively impaired patient may forget instructions.
A delirious patient may resist care.
An impulsive patient may fall.
A fatigued patient may give up early.
The psychiatrist helps the rehabilitation team by improving motivation, emotional stability, sleep, cognition, family communication and realistic goal-setting.
This is why psychiatry should not be seen as a “last resort” after stroke. It should be integrated early when mood, behaviour or cognition interferes with recovery.
10. Suicide risk assessment after stroke
Stroke can be emotionally devastating. Some patients experience sudden loss of independence, speech, mobility, work identity or dignity.
A psychiatrist is especially important when the patient says:
“I am a burden.”
“There is no point living.”
“I cannot live like this.”
“I wish I had died.”
Post-stroke depression, severe disability, social isolation, chronic pain, insomnia and hopelessness can increase suicide risk.
The psychiatrist assesses risk, builds a safety plan, involves the family, treats depression and anxiety, and helps the patient reconnect with achievable goals.
11. Family and caregiver counselling
Stroke changes the entire family system.
Caregivers may suddenly become responsible for medicines, feeding, toileting, physiotherapy, finances, hospital visits and emotional support. They may feel guilt, anger, exhaustion, resentment or helplessness.
A psychiatrist helps caregivers understand:
what is neurological,
what is psychiatric,
what is behavioural,
what is modifiable,
and what expectations are realistic.
Caregiver guidance may include:
how to communicate with aphasia,
how to encourage without criticising,
how to handle emotional outbursts,
how to structure routine,
how to reduce falls and impulsivity,
how to identify depression or delirium,
and when to seek urgent help.
A supported caregiver becomes part of treatment.
12. Medication review and safety
After stroke, patients may be on antiplatelets, anticoagulants, antihypertensives, statins, diabetes medicines, pain medicines and sleep medicines. Psychiatric medication must therefore be chosen carefully.
A psychiatrist considers:
bleeding risk with SSRIs and antiplatelets or anticoagulants,
hyponatraemia risk in older adults,
sedation and falls,
seizure threshold,
drug interactions,
cognitive side effects,
QT prolongation,
constipation,
urinary retention,
and blood pressure effects.
Good psychiatric care is not just adding tablets. It is choosing safely within the context of stroke, age, medical comorbidity and rehabilitation goals.
13. Helping with identity, grief and adjustment
Stroke can suddenly change a person’s life story.
A working professional may lose confidence.
A parent may feel dependent on children.
A spouse may feel embarrassed by speech difficulty.
A previously independent elder may feel humiliated needing help for bathing or toileting.
The psychiatrist helps patients process grief, anger, shame, fear, dependency and role change.
This is not merely “counselling.” It is part of recovery.
Physical recovery asks: Can the person walk?
Psychiatric recovery asks: Can the person live with meaning again?
Both are necessary.
14. Working with the stroke team
The ideal model is multidisciplinary.
The neurologist manages acute stroke diagnosis, secondary prevention and neurological follow-up.
The physician manages diabetes, hypertension, cardiac risk and medical comorbidity.
The physiotherapist works on mobility and strength.
The occupational therapist works on daily function.
The speech therapist works on speech and swallowing.
The psychiatrist manages mood, behaviour, cognition, sleep, motivation, delirium, medication safety and caregiver distress.
Together, the team can help the patient recover not only physically, but also emotionally and socially.
When should a stroke survivor see a psychiatrist?
A psychiatric consultation is useful if the patient has:
persistent sadness, crying spells or hopelessness,
excessive fear, panic or anxiety,
poor sleep or severe fatigue,
loss of motivation,
refusal of rehabilitation,
irritability or aggression,
suspiciousness or hallucinations,
confusion or delirium,
memory or judgement problems,
emotional outbursts,
suicidal thoughts,
difficulty adjusting to disability,
or caregiver burnout.
Early help can prevent complications and improve rehabilitation participation.
Summary :
The psychiatrist’s role in stroke management is central to whole-person recovery. A stroke may damage movement, speech or balance, but it can also disrupt mood, identity, cognition, behaviour and relationships.
A patient may need physiotherapy to stand again.
They may need speech therapy to communicate again.
They may need medical care to prevent another stroke.
But they may also need psychiatric care to regain hope, motivation, emotional stability and dignity.
For families, the message is simple:
If a stroke survivor develops depression, anxiety, sleep disturbance, confusion, memory problems, behavioural change or caregiver distress, psychiatric care can make a meaningful difference.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808