Dextromethorphan–Bupropion for Alzheimer’s Agitation: A New Non-Antipsychotic Chapter in Dementia Care
 Agitation in Alzheimer’s disease is one of the most distressing and difficult symptoms faced by patients, families, caregivers, and clinicians. It is not merely “difficult behaviour.” It may reflect fear, misperception, pain, sleep disruption, environmental overstimulation, delirium, medication adverse effects, caregiver mismatch, or progression of brain disease.
Agitation in Alzheimer’s disease is one of the most distressing and difficult symptoms faced by patients, families, caregivers, and clinicians. It is not merely “difficult behaviour.” It may reflect fear, misperception, pain, sleep disruption, environmental overstimulation, delirium, medication adverse effects, caregiver mismatch, or progression of brain disease.
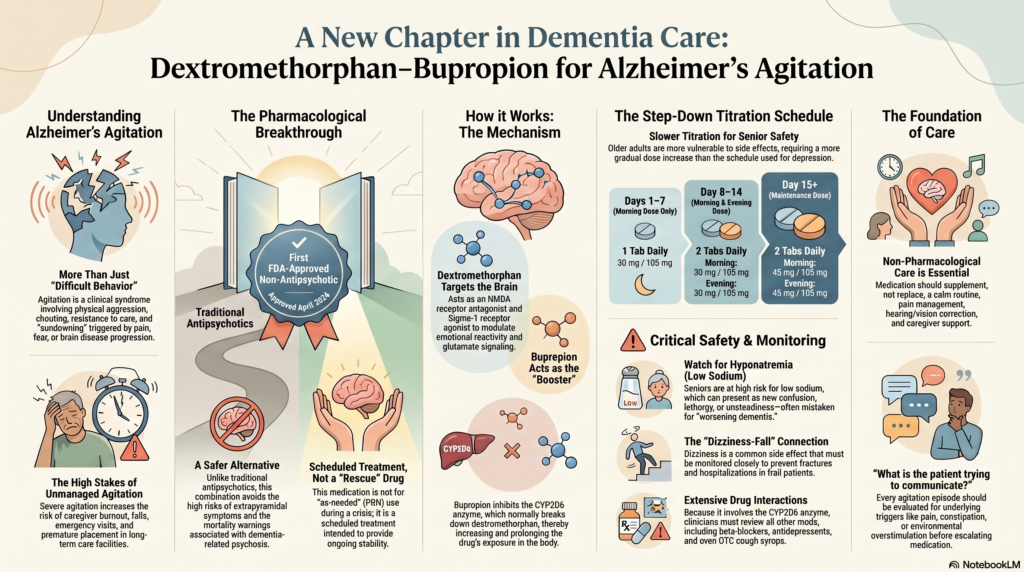
In April 2026, the U.S. FDA approved the fixed-dose combination of dextromethorphan hydrobromide and bupropion hydrochloride for the treatment of agitation associated with dementia due to Alzheimer’s disease. This is clinically important because it is the first FDA-approved non-antipsychotic medication for this indication, and the second FDA-approved medication overall after brexpiprazole.
This approval does not mean every patient with dementia-related agitation should receive this medication. But it expands the treatment conversation beyond the traditional reliance on sedatives and antipsychotics.
Why agitation in Alzheimer’s disease matters
Agitation in Alzheimer’s disease may include:
- Restlessness and pacing
- Repeated shouting or verbal aggression
- Irritability and emotional distress
- Resistance to care
- Physical aggression
- Disinhibition
- Sleep-wake disruption
- Suspiciousness or fear-driven behaviour
- Evening worsening, often described as “sundowning”
For families, agitation is often the point where home care becomes extremely difficult. It increases caregiver burnout, worsens quality of life, and may lead to earlier institutionalisation. It can also increase the risk of falls, injury, emergency visits, and unnecessary medication use.
Agitation should therefore be understood as a clinical syndrome, not just a behavioural inconvenience.
What is dextromethorphan–bupropion?
This combination is interesting because it is not a conventional sedative, benzodiazepine, or antipsychotic.
Dextromethorphan has activity at several brain targets, including:
- NMDA receptor antagonism
- Sigma-1 receptor agonism
- Effects on glutamatergic signalling
- Modulation of emotional and behavioural reactivity
Bupropion is included partly because it inhibits CYP2D6, the enzyme that rapidly metabolises dextromethorphan. By inhibiting CYP2D6, bupropion increases and prolongs dextromethorphan exposure.
Bupropion also has noradrenergic and dopaminergic activity. This is clinically relevant because it means clinicians must watch for insomnia, agitation, blood pressure changes, seizure risk, and drug interactions.
The exact mechanism by which this combination reduces Alzheimer’s agitation is not fully established, but it is thought to involve modulation of glutamate, sigma-1 receptor pathways, and neurobehavioural circuits involved in emotional regulation and behavioural control.
Why this approval is different
Until recently, pharmacological management of Alzheimer’s agitation relied heavily on off-label approaches such as:
- Antipsychotics
- Antidepressants
- Anticonvulsants
- Benzodiazepines
- Sedative-hypnotics
- Cholinesterase inhibitor or memantine optimisation
- Environmental and behavioural strategies
Brexpiprazole became the first FDA-approved medication for agitation associated with dementia due to Alzheimer’s disease. Dextromethorphan–bupropion now adds a second approved option — and importantly, from a non-antipsychotic pharmacological class.
This matters because antipsychotics in dementia carry important concerns, including sedation, extrapyramidal symptoms, falls, cerebrovascular events, metabolic effects, and mortality warnings in elderly patients with dementia-related psychosis.
A non-antipsychotic option may therefore be useful in selected patients. However, “non-antipsychotic” does not mean “risk-free.” It requires careful patient selection, dose titration, and monitoring.
Dosing: different from the depression schedule
One of the most practical points is that the Alzheimer’s agitation titration schedule differs from the schedule used for major depressive disorder.
For agitation associated with dementia due to Alzheimer’s disease, the approved titration schedule uses a lower-strength tablet initially and proceeds gradually.
A typical schedule is:
| Time period | Dose |
|---|---|
| Days 1–7 | Dextromethorphan 30 mg / bupropion 105 mg once daily in the morning |
| Day 8 onward | Dextromethorphan 30 mg / bupropion 105 mg twice daily, at least 8 hours apart, if tolerated |
| Day 15 onward | Dextromethorphan 45 mg / bupropion 105 mg twice daily, at least 8 hours apart, if tolerated |
The tablets should be swallowed whole and should not be crushed, divided, or chewed. The total daily dose should not exceed the approved maximum.
This slower titration is important because older adults with dementia are more vulnerable to dizziness, falls, confusion, drug interactions, renal impairment, and electrolyte disturbances.
Not a PRN medication
A major clinical point: dextromethorphan–bupropion is not intended as an as-needed or PRN medication for agitation.
It is not a rescue sedative for sudden aggression. It is a scheduled medication intended for ongoing treatment of agitation associated with Alzheimer’s dementia.
This distinction matters in real-world practice. Families often ask for a medicine to “give only when the patient becomes aggressive.” That is a different clinical situation.
Acute agitation, especially when there is danger to the patient or others, requires immediate assessment of triggers, safety, delirium, pain, infection, environmental factors, and sometimes emergency management.
Dextromethorphan–bupropion should be viewed as part of a structured treatment plan, not a crisis-control tablet.
What did the clinical trials show?
The approval was supported by clinical trial data showing benefit in agitation symptoms.
In an acute treatment study, patients with Alzheimer’s agitation who received dextromethorphan–bupropion showed improvement in agitation severity compared with placebo. Agitation was assessed using standardised instruments such as the Cohen-Mansfield Agitation Inventory, which evaluates behaviours such as verbal aggression, physical aggression, restlessness, pacing, and resistance to care.
In a longer-term relapse-prevention study, patients who had responded to treatment were continued on medication or switched to placebo. Those who continued treatment had a longer time to relapse of agitation symptoms.
This is clinically meaningful because Alzheimer’s agitation often has a relapsing and fluctuating course. Acute improvement is important, but maintaining stability is equally important for caregiver confidence, home care, and long-term planning.
Adverse effects in Alzheimer’s agitation may differ from depression
The adverse-effect profile in older adults with Alzheimer’s agitation may differ from that seen in younger or middle-aged adults treated for depression.
In the Alzheimer’s agitation population, particular attention should be paid to:
- Dizziness
- Dyspepsia
- Falls
- Confusion or worsening cognition
- Sleep disturbance
- Blood pressure changes
- Hyponatremia
- Drug interactions
- Seizure risk
- Serotonin syndrome risk when combined with serotonergic medicines
Dizziness is especially important in dementia care. A seemingly mild side effect can translate into falls, fractures, hospitalisation, immobility, and further cognitive decline.
The hyponatremia warning is especially relevant in older adults
One of the important safety considerations in the 2026 label is hyponatremia, or low serum sodium.
This matters because older adults with dementia often have multiple risk factors for hyponatremia, including:
- Low baseline sodium
- Diuretic use
- SSRI or SNRI use
- Poor oral intake
- Dehydration
- Frailty
- Intercurrent infections
- Chronic kidney disease
- Polypharmacy
In dementia, hyponatremia may present as:
- Sudden worsening confusion
- Increased agitation
- Lethargy
- Unsteadiness
- Falls
- Seizures
- New hallucinations
- Reduced alertness
A major mistake in dementia care is to assume that every sudden behavioural change is “progression of dementia.” New confusion or agitation should always trigger a search for reversible medical causes, including electrolyte abnormalities.
CYP2D6: a practical prescribing issue
CYP2D6 is central to this medication.
Bupropion inhibits CYP2D6, thereby increasing dextromethorphan exposure. But this also creates interaction concerns.
Clinicians must review other medications carefully, especially:
- Strong CYP2D6 inhibitors
- Other bupropion-containing products
- Other dextromethorphan-containing products
- SSRIs such as fluoxetine or paroxetine
- Tricyclic antidepressants
- Antipsychotics metabolised by CYP2D6
- Beta-blockers such as metoprolol
- Opioids such as codeine or tramadol
- Medicines that lower seizure threshold
- Other serotonergic drugs
This is especially important in dementia because patients may already be receiving multiple medications from different specialists. Over-the-counter cough syrups containing dextromethorphan should also be specifically checked.
Polypharmacy review is not a formality; it is a core safety step.
Dose adjustments and special populations
Dose adjustment is important in selected patients.
The maximum recommended dose is lower in:
- Moderate renal impairment
- Patients receiving strong CYP2D6 inhibitors
- Known CYP2D6 poor metabolisers
This matters because renal impairment is common in older adults, and CYP2D6 interactions are easy to miss.
In frail elderly patients, the principle should be:
Start carefully, titrate slowly, monitor closely, and reassess frequently.
Who needs extra caution?
Dextromethorphan–bupropion may not be suitable for every patient with Alzheimer’s agitation.
Extra caution is needed in patients with:
- History of seizure disorder
- Eating disorders such as anorexia nervosa or bulimia
- Abrupt alcohol, benzodiazepine, barbiturate, or antiepileptic withdrawal
- Severe head injury
- Stroke-related brain injury
- CNS tumour or CNS infection
- Uncontrolled hypertension
- Bipolar disorder or history of mania/hypomania
- Active psychosis requiring antipsychotic treatment
- High fall risk
- Significant renal impairment
- Baseline hyponatremia
- Multiple serotonergic medications
- Multiple drugs that lower seizure threshold
- Frailty, dehydration, or poor oral intake
A non-antipsychotic medication is not automatically safer for every patient. The safety profile is different, not absent.
Screening before starting treatment
Before starting medication for Alzheimer’s agitation, the clinician should ask a basic but vital question:
Why is the patient agitated?
Agitation may be due to dementia itself, but it may also be due to treatable causes such as:
- Pain
- Constipation
- Urinary retention
- Urinary tract infection
- Pneumonia
- Dehydration
- Hypoxia
- Delirium
- Sleep deprivation
- Medication adverse effects
- Benzodiazepine or alcohol withdrawal
- Environmental overstimulation
- Fear during bathing, dressing, or toileting
- Caregiver communication mismatch
A good pre-treatment assessment should include:
- Confirmation of dementia diagnosis and likely Alzheimer’s aetiology
- Assessment of agitation severity, frequency, triggers, and risks
- Review of all prescription, over-the-counter, and herbal medications
- Blood pressure assessment
- Renal function assessment
- Serum sodium and electrolytes, especially in high-risk patients
- History of seizures, falls, mania, substance use, and medication sensitivity
- Assessment of caregiver capacity and safety
- Evaluation for delirium and acute medical illness
- Documentation of target symptoms before starting medication
The last point is important. Without defining the target symptoms, it becomes difficult to know whether the medication is truly helping.
Monitoring after initiation
Once started, monitoring should be practical and caregiver-friendly.
Families can be asked to track:
- Number of agitation episodes per day
- Timing of episodes
- Triggers
- Sleep pattern
- Physical aggression
- Verbal aggression
- Resistance to care
- Wandering or pacing
- Falls or near-falls
- Dizziness
- Appetite and hydration
- New confusion
- Excessive sleepiness
- Tremor, sweating, diarrhoea, fever, or rigidity
- Any sudden neurological change
Clinicians should monitor:
- Blood pressure
- Sodium in high-risk patients
- Renal function where relevant
- Drug interactions after every medication change
- Emergence of manic or psychotic symptoms
- Seizure risk
- Overall caregiver burden
- Need for continuation, dose adjustment, or discontinuation
In dementia care, caregiver observation is often more valuable than a brief clinic snapshot.
Non-pharmacological care remains essential
This approval should not reduce the importance of behavioural and environmental care.
Medication may reduce agitation, but it cannot replace:
- A calm and predictable routine
- Good sleep hygiene
- Pain management
- Constipation management
- Hearing and vision correction
- Simplified communication
- Avoidance of confrontation
- Reducing noise and overstimulation
- Structured daytime activity
- Caregiver education
- Safety planning
- Support for caregiver burnout
A helpful principle is:
Do not ask only, “Which medicine will calm the patient?”
Ask, “What is the patient trying to communicate through agitation?”
Relevance for Indian clinical practice
For clinicians and families in India, it is important to remember that this is a U.S. FDA approval. Availability, regulatory approval, pricing, and approved indications in India may differ.
Indian dementia care has its own realities:
- Delayed diagnosis
- Limited access to geriatric psychiatry
- High family caregiver burden
- Polypharmacy
- Overuse of sedatives
- Under-recognition of delirium
- Limited respite care
- Stigma around behavioural symptoms
- Difficulty maintaining structured follow-up
Any new medication must therefore be integrated into a broader dementia care model rather than used in isolation.
In the Indian setting, the foundation remains:
- Accurate diagnosis
- Caregiver psychoeducation
- Medical review for reversible causes
- Behavioural and environmental modification
- Judicious medication use
- Regular follow-up
- Safety planning
- Support for caregiver distress
Final clinical takeaway
Dextromethorphan–bupropion represents an important shift in the treatment of agitation associated with Alzheimer’s dementia. It offers a scheduled, non-antipsychotic, mechanism-driven option with evidence for reducing agitation and delaying relapse in selected patients.
But it should not be seen as a simple calming tablet.
It requires:
- Correct diagnosis
- Careful patient selection
- Slow titration
- Drug-interaction review
- Sodium and renal monitoring where relevant
- Blood pressure monitoring
- Attention to CYP2D6
- Fall-risk assessment
- Caregiver education
- Continued behavioural and environmental management
The future of dementia care will not be “drug versus no drug.” It will be precision-informed, caregiver-supported, symptom-specific care — where medications are used thoughtfully, not reflexively.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- Bupropion-Dextromethorphan Combination
- Bupropion-Dextromethorphan Combination for Depression: A Comprehensive Review
- Geriatric Care : How to Care for an Elderly Person With Dementia at Home
- Dementia Series: The Role of Technology in Dementia Care – Innovations for Better Support
- Dementia Series: End-of-Life Care in Dementia – Providing Comfort and Dignity
- Dementia Series: Young-Onset Dementia – When Dementia Strikes Early