P-SPIKES: A Practical Model for Breaking Bad News
 SP-SPIKES is a modified version of the well-known SPIKES protocol for breaking bad news. The original SPIKES model includes Setting, Perception, Invitation, Knowledge, Emotions/Empathy, Strategy/Summary and was developed as a structured method for difficult medical conversations.
SP-SPIKES is a modified version of the well-known SPIKES protocol for breaking bad news. The original SPIKES model includes Setting, Perception, Invitation, Knowledge, Emotions/Empathy, Strategy/Summary and was developed as a structured method for difficult medical conversations.
The added “P” stands for Preparation — because bad news should never be delivered casually, hurriedly, or without emotional and factual readiness.
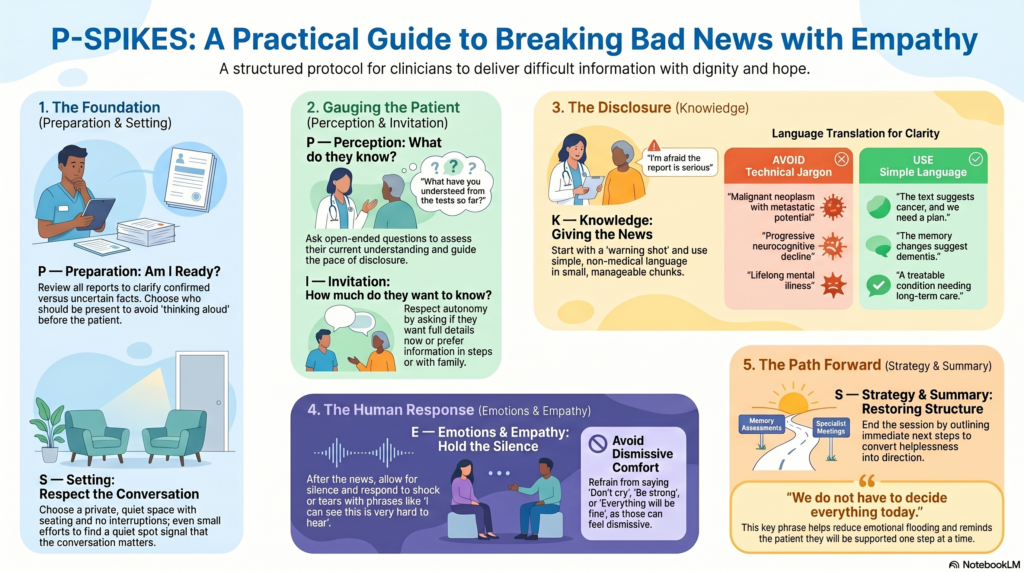
What P-SPIKES Stands For
| Step | Meaning | Core Question |
|---|---|---|
| P | Preparation | Am I ready with the facts, setting, and emotional composure? |
| S | Setting | Is the place private, calm, and respectful? |
| P | Perception | What does the patient/family already understand? |
| I | Invitation | How much does the patient want to know now? |
| K | Knowledge | How do I share the information clearly and gently? |
| E | Emotions/Empathy | How do I respond to shock, silence, anger, tears, or denial? |
| S | Strategy/Summary | What is the next step, and how do I preserve realistic hope? |
P — Preparation
Before speaking to the patient, the doctor must prepare.
This includes:
- Reviewing diagnosis, reports, prognosis, and treatment options.
- Clarifying what is confirmed and what is still uncertain.
- Choosing who should be present.
- Preparing for emotional reactions.
- Ensuring enough time is available.
A common mistake is to enter the room with half-formed facts and then “think aloud” in front of the patient. Bad news requires honesty, but also precision.
Useful self-check:
“What exactly do I know?”
“What do I not yet know?”
“What is the safest and kindest way to explain this?”
S — Setting
Bad news should ideally be shared in a private, quiet space. Sit down. Avoid phone interruptions. Maintain eye contact. Do not stand at the doorway and deliver life-changing information.
In Indian hospitals, space and time constraints are real. Even then, a small effort matters:
“Let us sit somewhere quieter. I need to explain the report properly.”
The setting itself tells the patient: “This conversation matters.”
P — Perception
Before giving information, assess what the patient or family already knows.
Ask:
“What have you understood from the tests so far?”
“What are you most worried about?”
“Has anyone explained the report to you?”
This step prevents unnecessary shock. Sometimes the patient already suspects the diagnosis. Sometimes the family knows more than the patient. Sometimes everyone is confused.
Perception guides the pace of disclosure.
I — Invitation
Not every patient wants the same amount of information at the same time. Some want all details. Some want only the broad picture. Some prefer family involvement.
Ask:
“Would you like me to explain the full details now?”
“Would you prefer that I speak with you alone or with your family?”
“Shall I explain step by step?”
This respects autonomy and reduces emotional flooding.
K — Knowledge
Now share the bad news clearly.
Use a warning shot first:
“I am afraid the report is more serious than we expected.”
“I have some difficult news to share.”
Then use simple language.
Instead of:
“There is a malignant neoplasm with metastatic potential.”
Say:
“The test suggests cancer, and we need to plan treatment quickly.”
Instead of:
“There is progressive neurocognitive decline.”
Say:
“The memory changes are more than normal ageing. The pattern suggests dementia.”
Give information in small chunks. Pause frequently. Check understanding.
“Would you like me to pause for a moment?”
“Is this making sense so far?”
E — Emotions and Empathy
After the news, the most important intervention is often silence.
Do not rush immediately into treatment details. The patient may not hear anything after the first emotional blow.
Helpful empathic responses:
“I can see this is very hard to hear.”
“I wish the news were different.”
“Please take your time.”
“Your reaction is understandable.”
“We are here with you.”
The Indian Journal of Psychiatry clinical practice guideline also emphasizes that breaking bad news requires sensitivity to emotional reactions, patient preferences, family dynamics, and cultural context.
Avoid:
“Don’t cry.”
“Be strong.”
“Everything will be fine.”
“At least it is not worse.”
“You should have come earlier.”
These may sound supportive but can feel dismissive.
S — Strategy and Summary
Bad news should not end with emotional collapse. The clinician must gently restore structure.
Say:
“We do not have to decide everything today.”
“The next step is…”
“I will write down the plan.”
“We will take this one step at a time.”
This final step converts helplessness into direction.
For example:
“The scan suggests dementia. The next step is to assess memory, daily functioning, mood, sleep, and safety. We will also discuss medicines, cognitive stimulation, family support, and long-term planning.”
Or:
“The diagnosis appears to be bipolar disorder. This does not mean life is over. It means we need a long-term plan to prevent mood episodes, protect sleep, and maintain functioning.”
P-SPIKES in One Clinical Script
“I have reviewed the reports carefully. Before I explain them, can you tell me what you have understood so far?”
“I am afraid the result is more serious than we hoped.”
“The scan shows a growth. We are concerned that it may be cancer.”
“I can see this is shocking. Please take your time.”
“We do not have to decide everything immediately. The next step is to confirm the type and meet the oncology team. I will help you understand each stage.”
P-SPIKES in Psychiatry
In psychiatry, bad news may not always be a death sentence, but it can feel like an identity sentence.
Examples include:
- Telling a family that a parent has dementia.
- Explaining schizophrenia or bipolar disorder to a young adult.
- Discussing autism or intellectual disability with parents.
- Explaining relapse in addiction.
- Telling a patient that long-term treatment may be needed.
- Discussing suicide risk with family.
Psychiatric bad news must be delivered with special care because stigma, shame, guilt, and fear are often intense.
Better language:
“This is a treatable condition, but it needs structured long-term care.”
Instead of:
“This is lifelong mental illness.”
Say:
“This condition may need ongoing monitoring, but many people recover functionally with the right treatment and support.”
Key Takeaway
P-SPIKES = Preparation + SPIKES.
It reminds us that difficult conversations are not spontaneous announcements. They are clinical procedures requiring preparation, empathy, clarity, and follow-through.
Bad news cannot always be softened. But it can be delivered in a way that preserves dignity, trust, and hope.
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
Related posts:
- When Bad Dreams Don’t Let Go – Understanding Nightmare Disorder
- Suicide Prevention & Mental Health Awareness: Breaking the Stigma
- Emotional Health in Men: Breaking the Silence, Rebuilding Strength in Chennai
- Breaking the Cycle: An Introduction to Cognitive Behavioural Therapy (CBT)
- The Big Five Personality Traits (OCEAN Model): Understanding Human Behavior
- Metacognitive Model of Anxiety