Phenocopy of Autism: A QEEG Exploration and Revelation
 In contemporary psychiatric practice, clinicians are increasingly encountering individuals—often intelligent, introspective, and high-functioning—who present with autism-like features in adolescence or adulthood. Social withdrawal, sensory sensitivity, mental fatigue, rigidity, and difficulty sustaining engagement raise an important question:
In contemporary psychiatric practice, clinicians are increasingly encountering individuals—often intelligent, introspective, and high-functioning—who present with autism-like features in adolescence or adulthood. Social withdrawal, sensory sensitivity, mental fatigue, rigidity, and difficulty sustaining engagement raise an important question:
Is this Autism Spectrum Disorder, or is something else mimicking it?
This is where the concept of phenocopy of autism becomes clinically vital—and where quantitative EEG (QEEG) adds clarity beyond symptom checklists.
What Is a Phenocopy of Autism?
A phenocopy refers to a clinical presentation that resembles a disorder phenomenologically, but does not share the same underlying neurodevelopmental mechanism.
In the case of autism, a phenocopy may look like:
-
social selectivity or withdrawal
-
reduced emotional expressiveness
-
sensory hypersensitivity
-
preference for predictability
-
cognitive rigidity
-
attentional effort and fatigue
Yet critically, these features:
-
emerge later in life, and
-
are state-dependent, not developmentally fixed.
Depression, anxiety, burnout, trauma, and incomplete affective remission are among the most common causes of autism phenocopies.
Why “Level 1 Autism” Is Often Invoked
DSM-5’s “Level 1 Autism” is frequently misunderstood as “mild autism” or “autistic traits.” In reality, it still requires:
-
early developmental onset,
-
persistent social-communication differences, and
-
restricted or repetitive behaviors across the lifespan.
When autism-like features appear after adolescence, especially following mood disorders, the neurodevelopmental logic of ASD becomes questionable—no matter how convincing the surface phenotype appears.
Where QEEG Becomes Revelatory
Symptom scales can blur boundaries.
Developmental history can be ambiguous.
QEEG helps at the level of brain network dynamics.
Typical QEEG patterns in Autism Spectrum Disorder often show:
-
early and stable network-level connectivity differences
-
altered coherence patterns
-
sensorimotor rhythm (mu) abnormalities
-
atypical hemispheric specialization
These patterns tend to be trait-like and developmentally anchored.
QEEG Patterns in Autism Phenocopies
In contrast, individuals with depression-related or anxiety-related phenocopies often show:
-
default mode network (DMN) dominance
-
elevated frontal or right-hemispheric alpha
-
inefficient rest-to-task state switching
-
preserved regulatory symmetry
-
intact executive control despite high cognitive effort
This pattern reflects an internally preoccupied brain, not a developmentally rewired one.
The person feels autistic—socially drained, sensory-overloaded, cognitively rigid—while the brain data reveals state-dependent inefficiency rather than structural difference.
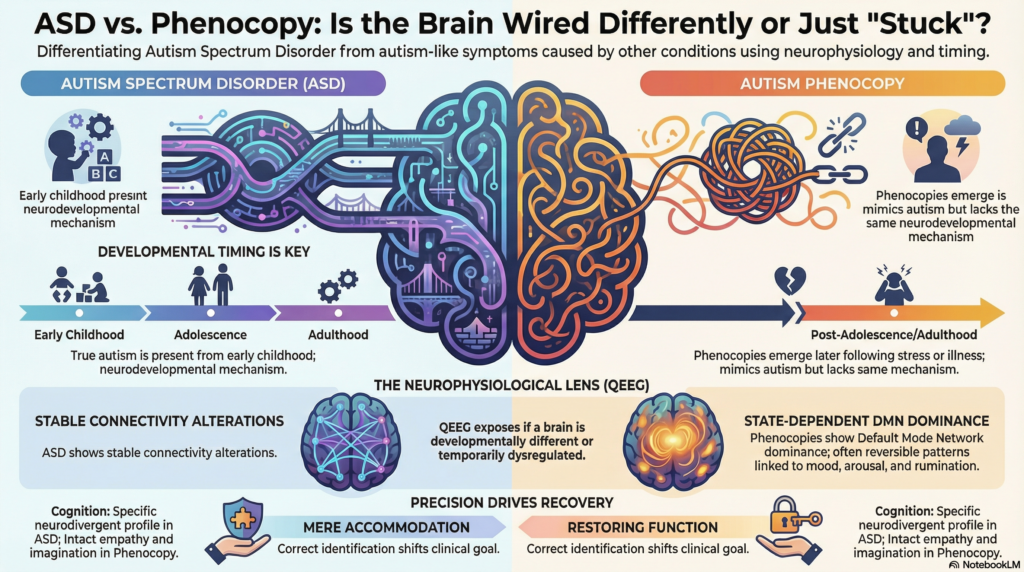
The Key Insight: Timing + Physiology
The most reliable differentiation rests on two pillars:
-
Developmental timing
-
Autism: present from early childhood
-
Phenocopy: emerges after emotional illness, stress, or burnout
-
-
Neurophysiology
-
Autism: stable, trait-like network alterations
-
Phenocopy: reversible patterns linked to mood, arousal, and rumination
-
QEEG does not “diagnose” autism—but it exposes whether the brain is developmentally different or temporarily dysregulated.
Why This Distinction Matters
Mislabeling a phenocopy as autism can:
-
obscure treatable depression or anxiety
-
lead to therapeutic pessimism
-
reinforce fixed identity narratives
-
shift care from recovery to mere accommodation
Recognizing a phenocopy reframes the clinical goal:
not coping with difference, but restoring function.
The Clinical Revelation
When autism-like features coexist with:
-
intact childhood social development
-
preserved empathy and imagination
-
strong objective cognitive performance
-
QEEG showing DMN dominance rather than connectivity disruption
the most parsimonious conclusion is not autism—but an autism phenocopy driven by affective neurophysiology.
This is not diagnostic minimization.
It is diagnostic precision.
Final Thought
Sometimes, the brain is not differently wired.
It is stuck in the wrong mode.
And when that is recognized, the path forward becomes clearer—and far more hopeful.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
Dr. Srinivas specializes in brain-based diagnostics using QEEG and neurocognitive profiling to differentiate ADHD, autism, and affective disorders, with a focus on avoiding over-pathologization and enabling meaningful recovery.
📞 +91-8595155808
✉ srinivasaiims@gmail.com