Why Psychiatrists Interrupt During a Consultation—and Why It May Be Good Clinical Practice
 Many patients enter a psychiatric consultation carrying months or even years of distress. They may have thought carefully about what they want to say, rehearsed the history repeatedly, or waited a long time for someone to hear the complete story.
Many patients enter a psychiatric consultation carrying months or even years of distress. They may have thought carefully about what they want to say, rehearsed the history repeatedly, or waited a long time for someone to hear the complete story.
It is therefore understandable that an interruption from the psychiatrist can feel uncomfortable.
A patient may wonder:
- “Why is the doctor not allowing me to finish?”
- “Has the psychiatrist already made up their mind?”
- “Does the doctor think my experience is unimportant?”
- “Am I being rushed?”
- “Why are we discussing sleep or substances when my real problem is my relationship?”
Sometimes these concerns are justified. A clinician who repeatedly interrupts out of impatience, distraction or lack of interest is not conducting a good interview.
However, not every interruption represents poor listening.
In psychiatric practice, careful redirection and focused interruption are often necessary diagnostic tools. The psychiatrist is not only listening to a story. The psychiatrist is also reconstructing chronology, clarifying the exact nature of symptoms, distinguishing between similar-looking conditions, evaluating safety and deciding what information must be prioritised before a treatment plan can be made.
An uninterrupted narrative may be emotionally meaningful while still being diagnostically incomplete.
The real question is therefore not simply:
“Did the psychiatrist interrupt?”
It is:
“Why did the psychiatrist interrupt, how was it done, and did it improve or weaken the assessment?”
A psychiatric interview is not an ordinary conversation
In everyday conversation, one person may listen while the other speaks freely. The purpose may be emotional expression, reassurance, companionship or mutual understanding.
A psychiatric diagnostic interview has a broader responsibility.
The psychiatrist must simultaneously:
- Understand the patient’s subjective experience
- Identify clinically significant symptoms
- Establish when the symptoms began
- Determine how they have changed over time
- Assess functioning
- Review previous treatment
- Consider medical and neurological explanations
- Evaluate substance use
- Examine risk
- Observe the patient’s mental state
- Develop a differential diagnosis
- Begin treatment planning
These tasks cannot always be completed through passive listening alone.
A person’s spontaneous account is invaluable because it reveals what matters most to them, how they organise their experience, what they fear, what they emphasise and what meaning they assign to events.
But spontaneous accounts do not necessarily follow diagnostic chronology.
Patients naturally tell stories according to emotional importance. Psychiatry must also organise those stories according to clinical relevance.
Emotional chronology and diagnostic chronology are different
A patient may begin with an argument that occurred the previous evening because it was emotionally painful. The psychiatrist may need to understand whether the argument was:
- A trigger for anxiety
- A consequence of irritability
- Part of a longstanding relationship pattern
- Related to alcohol use
- Associated with suspiciousness
- Occurring during a period of reduced sleep and increased energy
- One episode within a larger depressive or manic illness
The patient’s emotional chronology may be:
“My partner criticised me, I became upset, and nobody understands what I am going through.”
The diagnostic chronology may require answers to different questions:
- When did the irritability begin?
- Was it present before the relationship conflict?
- Has sleep changed?
- Is energy higher or lower?
- Has speech become more rapid?
- Have there been impulsive decisions?
- Has this happened in previous episodes?
- Is alcohol or another substance involved?
- Is there any risk of self-harm or aggression?
The psychiatrist may therefore interrupt a detailed description of the argument to establish the larger clinical sequence.
This does not necessarily mean that the relationship event is being dismissed. It means that the clinician is trying to determine what role it plays within the illness.
Why psychiatrists interrupt
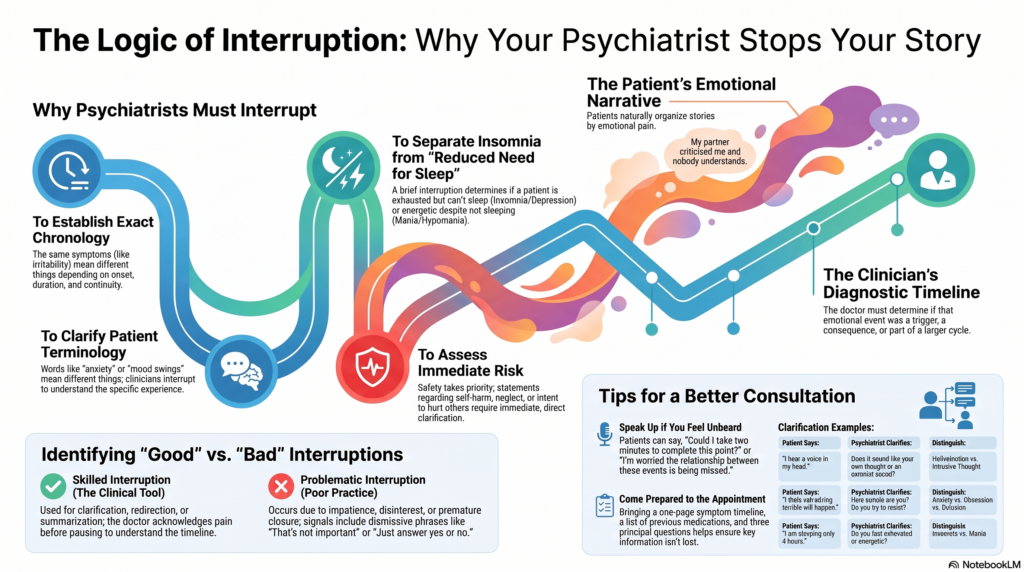
1. To establish chronology
Chronology is one of the most important components of psychiatric diagnosis.
The same symptoms can indicate very different conditions depending on:
- When they began
- How long they lasted
- Which symptom appeared first
- Whether symptoms were episodic or continuous
- Whether there was complete recovery between episodes
- Whether symptoms followed medication changes, substance use, childbirth, trauma or sleep deprivation
Consider a patient reporting poor concentration, irritability and low motivation.
These symptoms may occur in:
- Depression
- ADHD
- Anxiety
- Burnout
- Sleep deprivation
- Bipolar disorder
- Substance use
- Medication adverse effects
- Cognitive disorders
If the patient gives a long description of current workplace problems, the psychiatrist may interrupt to ask:
“Were these concentration difficulties present during childhood and school, or did they begin only in the last six months?”
That single question may substantially change the diagnostic direction.
Similarly, a patient describing “mood swings” may be interrupted with:
“How long does each mood change last—minutes, hours, days or weeks?”
Mood changes occurring several times within a day are clinically different from sustained episodes lasting several days or weeks.
Without chronology, psychiatric diagnosis becomes impressionistic.
2. To clarify what the patient means by a word
Patients and clinicians may use the same word while meaning very different things.
Common examples include:
- Anxiety
- Depression
- Panic
- Mood swings
- Overthinking
- Hallucination
- Paranoia
- Addiction
- Trauma
- Dissociation
- Obsession
- Memory loss
- Hyperactivity
When someone says, “I am anxious all the time,” the psychiatrist may need to interrupt and ask:
- Is it a physical sensation?
- Is there persistent worry?
- Are there sudden episodes of intense fear?
- Is there fear of losing control?
- Is the anxiety linked to intrusive thoughts?
- Is it mainly social fear?
- Is it related to traumatic memories?
- Is it actually internal restlessness caused by medication?
Likewise, “I have mood swings” may mean:
- Rapid emotional reactions to events
- Irritability
- Premenstrual changes
- Episodes of depression and mania
- Shifts related to substance use
- Emotional dysregulation
- Ordinary changes in mood across the day
A psychiatrist cannot safely diagnose from labels alone.
The clinician must understand the experience behind the word.
3. To distinguish thoughts from voices
Patients may say:
“I hear a voice in my head.”
That statement can refer to several distinct phenomena:
- An auditory hallucination
- An intrusive thought
- An internal monologue
- A vivid memory
- Dissociative self-talk
- Obsessional thinking
- Trauma-related re-experiencing
- A culturally interpreted spiritual experience
The psychiatrist may interrupt to ask:
- Does the experience feel like your own thought?
- Is it heard as if coming through the ears?
- Does it seem to originate inside or outside your head?
- Can you control it?
- Does it speak in the second or third person?
- Does it command you to do anything?
- Do you believe another person or force is producing it?
- Does it occur when falling asleep or waking up?
These are not trivial distinctions.
They can influence diagnosis, risk assessment, medication decisions and the need for urgent intervention.
Allowing the patient to continue using the general word “voice” without clarification may create serious diagnostic error.
4. To separate insomnia from reduced need for sleep
A patient may report:
“I am sleeping only four hours.”
This alone does not establish whether the person has insomnia, anxiety, depression, mania or simply an externally restricted sleep schedule.
The psychiatrist may interrupt to ask:
“After four hours of sleep, do you feel exhausted and wish you could sleep more, or do you feel energetic and believe you do not need additional sleep?”
The distinction is clinically important.
Insomnia
The person wants to sleep but cannot. They usually experience:
- Fatigue
- Irritability
- Poor concentration
- Daytime sleepiness
- Distress about not sleeping
Reduced need for sleep
The person sleeps less but does not feel tired. It may be accompanied by:
- Increased energy
- Increased activity
- Rapid speech
- Elevated or irritable mood
- Greater confidence
- Impulsive behaviour
- Increased social or sexual activity
Reduced need for sleep may be a significant feature of mania or hypomania.
A brief interruption can therefore prevent an important symptom from being misclassified.
5. To distinguish fear, obsession, overvalued belief and delusion
A patient may say:
“I think something terrible will happen.”
The psychiatrist must determine the nature of that belief.
Fear or worry
The person recognises uncertainty:
“I know it may not happen, but I keep worrying.”
Obsession
The thought is intrusive, repetitive and usually recognised as excessive or unwanted:
“I know it is irrational, but I cannot stop thinking that I may harm someone accidentally.”
Overvalued idea
The belief is strongly held and emotionally dominant, but some degree of doubt or discussion remains possible.
Delusion
The belief is held with fixed conviction despite strong contradictory evidence and may be part of a psychotic disorder.
The psychiatrist may therefore interrupt a lengthy explanation to ask:
- How certain are you?
- Is there any possibility that your interpretation may be mistaken?
- What evidence would change your mind?
- Do others agree with you?
- Does the thought feel unwanted?
- Do you try to resist it?
- How much time do you spend thinking about it?
These questions are not attempts to argue with the patient. They help classify the experience accurately.
6. To assess immediate risk
Risk assessment cannot always wait until the patient has finished the entire narrative.
Certain statements require immediate clarification:
- “I cannot continue like this.”
- “Everyone would be better without me.”
- “I wanted to teach him a lesson.”
- “The voices are asking me to do something.”
- “I have tablets stored at home.”
- “I have not eaten for several days.”
- “I have been driving at extreme speeds.”
- “I have not slept for four nights.”
- “I feel someone is about to attack me.”
The psychiatrist may interrupt to ask directly about:
- Suicidal thoughts
- Plans
- Intent
- Access to lethal means
- Previous attempts
- Risk to others
- Command hallucinations
- Severe self-neglect
- Impulsivity
- Intoxication
- Withdrawal
- Vulnerability to abuse
- Capacity to care for oneself
In such situations, continuing to listen without clarifying risk would not be respectful. It would be unsafe.
Safety takes priority over conversational smoothness.
7. To return to an unanswered question
Patients do not always answer the question that was asked.
This may happen because:
- The subject is uncomfortable
- The person misunderstood the question
- Anxiety caused them to lose track
- Attention is impaired
- Thoughts are racing
- The patient is avoiding a painful topic
- The narrative is highly circumstantial
- The person wishes to communicate a different priority
- Cognitive impairment affects recall
For example:
Psychiatrist: “Have you ever tried to harm yourself?”
Patient: “My family has never understood how much I have suffered. My father was very strict, and after marriage things became worse.”
The response may be clinically meaningful, but the risk question remains unanswered.
A responsible psychiatrist must return to it:
“I understand that the family situation has been painful, and we will discuss it. I also need a clear answer for your safety: have you ever attempted to harm yourself?”
That is not insensitivity. It is clinical responsibility.
8. To prevent key information from being lost in excessive detail
Some patients communicate in a highly detailed, circumstantial or tangential manner.
They may describe:
- Every message in an argument
- The complete history of several relationships
- Minor events from many years ago
- Repeated examples of the same symptom
- Extensive explanations of why others behaved badly
- Online research about a suspected diagnosis
- Every medication ever prescribed without clarifying the response
These details may matter, but not all of them carry equal diagnostic weight.
The psychiatrist may need to say:
“I can see that this event was important. To understand the clinical pattern, let us first establish when the sleep change began.”
Or:
“I will return to the relationship history. Before that, I need to clarify whether these symptoms occur only during conflicts or remain present even when things are going well.”
Without redirection, a consultation can become emotionally intense but diagnostically unfocused.
9. To distinguish symptoms from interpretations
Patients present both experiences and explanations.
An experience might be:
“My heart races, I sweat and feel I may faint in crowded places.”
The interpretation might be:
“I have a serious heart disease.”
Or:
“People are deliberately making me uncomfortable.”
The psychiatrist must respect the person’s interpretation while also separating it from the observable symptom pattern.
Another patient may say:
“I cannot focus because I definitely have ADHD.”
The psychiatrist still needs to assess:
- Childhood onset
- Cross-situational impairment
- Academic and occupational functioning
- Sleep
- Anxiety
- Depression
- Substance use
- Digital overuse
- Medical factors
- Learning difficulties
The interruption may therefore sound like:
“We will examine ADHD carefully. Before concluding, I need to establish whether the concentration difficulty was present before age 12 and whether it occurred in more than one setting.”
The psychiatrist is not rejecting the patient’s concern. The clinician is testing the diagnostic hypothesis.
10. To identify medical or substance-related causes
A psychiatric symptom does not always originate from a primary psychiatric disorder.
The psychiatrist may interrupt to ask about:
- Thyroid disease
- Seizures
- Head injury
- Menstrual or hormonal changes
- Sleep apnoea
- Steroid use
- Pain medication
- Alcohol
- Cannabis
- Stimulants
- Sedatives
- Caffeine
- Recent medication changes
A patient may feel that these questions are unrelated to their emotional problem. Clinically, they may be central.
Anxiety, agitation, psychosis, depression, cognitive changes and sleep disturbance can all be influenced by medical illness, medication or substance use.
A good psychiatric interview therefore resists the temptation to treat every psychological complaint as purely psychological.
Interruption, redirection and clarification are not the same
The word “interruption” often sounds negative. But several different clinical behaviours may be grouped under that term.
Clarification
“When you say you felt detached, did you feel detached from yourself, from the surroundings, or emotionally numb?”
The purpose is precision.
Redirection
“I understand the workplace conflict. Let us return to when the sleep difficulty first started.”
The purpose is organisation.
Summarising
“Let me check whether I have understood correctly: the anxiety began in January, worsened after the job change and is now associated with panic attacks.”
The purpose is accuracy.
Prioritisation
“Before we discuss treatment, I need to ask about the suicidal thoughts you mentioned.”
The purpose is safety.
Boundary-setting
“We may not be able to cover every historical event today. Let us focus first on the symptoms that require immediate treatment.”
The purpose is realistic clinical planning.
These are different from dismissive interruption, where the doctor changes the subject without acknowledging what the patient was trying to communicate.
When interruption becomes poor clinical practice
Not every interruption is justified.
Interruption becomes problematic when it arises from:
- Impatience
- Disinterest
- Distraction
- Stereotyping
- Premature diagnostic closure
- Excessive focus on completing a checklist
- Pressure to finish quickly
- Failure to tolerate emotional expression
- A desire to dominate the consultation
- Discomfort with trauma, grief, anger or sexuality
- Preoccupation with prescribing rather than understanding
Poor interruption may sound like:
- “That is not important.”
- “Just answer yes or no.”
- “You are overthinking.”
- “We do not have time for this.”
- “I already know what your problem is.”
- “There is no need to explain.”
Such statements can make patients feel silenced and may cause vital information to be missed.
A psychiatrist who interrupts repeatedly without summarising or acknowledging the patient’s concerns may create a technically structured but emotionally unsafe consultation.
How skilled psychiatrists interrupt
A good psychiatrist does not simply cut the patient off. The clinician signals that the patient has been heard and explains why redirection is necessary.
Useful phrases include:
“I can see that this has been very painful. I am going to pause you briefly so that I can understand the timeline.”
“That point is important, and I will return to it. Before we move on, I need to clarify what you meant by hearing a voice.”
“I do not want to lose the main clinical issue. Let me summarise what I have understood so far.”
“I am interrupting because the statement you made raises a safety concern.”
“There are several important parts to your story. Let us organise them one at a time.”
“I understand why you connect the symptoms to that event. I also need to check whether there were earlier episodes.”
These statements preserve both structure and dignity.
The ideal psychiatric interview moves from open to focused
A balanced diagnostic interview generally progresses through stages.
Stage 1: Open invitation
The psychiatrist begins with a broad question:
“What brought you for consultation?”
“Please tell me what has been troubling you.”
This allows the patient to describe the problem in their own language.
The spontaneous narrative reveals:
- The patient’s priorities
- Emotional tone
- Organisation of thought
- Insight
- Explanatory model
- Communication style
- Level of distress
Stage 2: Clarification
The psychiatrist begins asking more specific questions:
- When did it start?
- How often does it happen?
- How long does it last?
- What makes it better or worse?
- What happens before and after it?
- How does it affect work and relationships?
Stage 3: Differential diagnosis
The interview becomes more targeted:
- Any periods of increased energy?
- Any panic attacks?
- Any compulsions?
- Any substance use?
- Any psychotic symptoms?
- Any childhood attention problems?
- Any medical conditions?
Stage 4: Risk and functional assessment
The clinician examines:
- Suicide risk
- Self-harm
- Violence risk
- Self-neglect
- Driving or financial risk
- Occupational decline
- Relationship instability
- Capacity for daily functioning
Stage 5: Formulation and treatment planning
The psychiatrist summarises:
- The likely diagnosis
- Alternative possibilities
- Contributing factors
- Further investigations
- Medication options
- Psychological interventions
- Follow-up needs
The interview therefore begins broadly and progressively narrows.
Too much structure at the beginning can silence the patient. Too little structure throughout can produce an incomplete assessment.
Why a long story is not always a complete history
The amount of speech does not necessarily equal the amount of clinically usable information.
A patient may speak for forty minutes while leaving unanswered:
- When symptoms began
- Whether symptoms are episodic
- Whether substances are involved
- Whether there is suicidal risk
- Which medications were tried
- Whether childhood symptoms were present
- Whether functioning has declined
- Whether there are psychotic symptoms
Conversely, a focused twenty-minute interview may establish:
- A clear chronology
- The principal symptoms
- Relevant exclusions
- Immediate risk
- Functional impairment
- A provisional diagnosis
- A safe initial treatment plan
Consultation quality should therefore not be judged only by how long the patient spoke without interruption.
The more meaningful questions are:
- Was the patient’s main concern understood?
- Were essential symptoms assessed?
- Was safety evaluated?
- Was the clinical reasoning explained?
- Was there a coherent plan?
Listening is not the same as agreeing
Some patients feel unheard when the psychiatrist does not agree with their preferred explanation, diagnosis or treatment.
But listening means understanding the person’s account accurately. It does not require the clinician to endorse every conclusion drawn from that account.
A psychiatrist may listen carefully and still conclude that:
- The symptoms do not support ADHD
- Mood instability is not necessarily bipolar disorder
- A requested sedative is unsafe
- An internet-based tapering schedule is unsuitable
- Substance use is contributing to symptoms
- Relationship patterns require psychological treatment
- Further assessment is needed before diagnosing a personality disorder
- Medication alone will not solve the problem
Clinical disagreement is not automatically evidence of poor listening.
At the same time, the psychiatrist should explain the disagreement rather than simply dismissing the patient’s view.
The role of mental-status observation during the narrative
While the patient speaks, the psychiatrist is also conducting a mental-status examination.
The clinician may observe:
- Whether speech is unusually rapid or slow
- Whether answers are direct or circumstantial
- Whether thoughts remain connected
- Whether affect matches the subject discussed
- Whether the patient becomes suspicious
- Whether attention is sustained
- Whether memory is reliable
- Whether the person can consider alternative explanations
- Whether emotional regulation changes during disagreement
The way a history is narrated may itself provide information.
For example:
- Repeatedly losing track may suggest impaired attention or cognition.
- Extremely pressured speech may occur during mood elevation.
- Highly detailed but indirect answers may reflect anxiety, obsessionality or circumstantial thinking.
- Abrupt topic shifts may require assessment for thought disorder, distractibility or severe emotional arousal.
The psychiatrist may interrupt partly because the form of communication has become diagnostically relevant.
Cultural and linguistic sensitivity matters
Interruption is more likely to be misunderstood when the psychiatrist and patient differ in:
- Language
- Cultural background
- Social expectations
- Communication style
- Age
- Educational background
- Familiarity with psychiatric terminology
Some cultures value detailed contextual narration. Others favour direct answers. Some patients expect the doctor to take a highly authoritative role, while others expect extensive collaborative discussion.
Language barriers can also make clarification appear repetitive or abrupt.
A culturally sensitive psychiatrist should explain the structure of the interview and avoid assuming that indirect communication represents evasion or pathology.
What patients can do when they feel interrupted
A patient who feels that something important has not been heard can say:
“I understand that you need specific information, but there is one part of the story that I feel is essential.”
“Could I take two minutes to complete this point before we move on?”
“I am worried that the relationship between these events is being missed.”
“Could you explain why this question is important for the diagnosis?”
“Before the consultation ends, I would like to return to one concern.”
These are reasonable requests.
Patients may also bring:
- A one-page symptom timeline
- A list of previous medicines
- A summary of major episodes
- Relevant medical records
- Three principal questions
- Collateral information from a family member when appropriate
Preparation helps ensure that the most important information is not lost.
What psychiatrists should do before ending the consultation
Even when the interview has required frequent redirection, the psychiatrist should ideally close the consultation by summarising:
- The main concerns understood
- The likely diagnosis or possibilities
- Important areas of uncertainty
- Immediate risks
- The proposed treatment
- The need for further assessment
- The follow-up plan
A useful closing statement may be:
“You described several important concerns. The most clinically significant pattern appears to be persistent anxiety with panic symptoms, worsened by sleep disruption. I have not found sufficient evidence today for bipolar disorder, but we will continue to monitor the mood history. We also need to address alcohol use because it may be worsening the sleep and anxiety.”
This demonstrates that the psychiatrist has listened, organised the information and translated it into a clinical formulation.
Directness and empathy are not opposites
A psychiatrist can be compassionate without allowing the interview to become directionless.
Similarly, a psychiatrist can be direct without becoming disrespectful.
Good psychiatric interviewing requires both:
Empathy without loss of structure
The patient’s suffering is acknowledged, but the clinician still asks difficult questions.
Structure without loss of humanity
The psychiatrist obtains essential information without reducing the person to a checklist.
Directness without humiliation
The clinician names risks, contradictions and maladaptive patterns without attacking the patient’s character.
Listening without passive agreement
The psychiatrist understands the patient’s viewpoint while retaining independent clinical judgement.
This balance distinguishes professional interviewing from either casual conversation or mechanical interrogation.
When interruption protects the patient
At its best, clinical interruption serves one of four purposes:
It clarifies
The psychiatrist identifies what the symptom actually is.
It organises
The clinician reconstructs the sequence of events.
It differentiates
Similar-looking disorders are separated from one another.
It protects
Urgent risk, medical causes and unsafe treatment requests are addressed.
Interruption becomes clinically justified when it improves accuracy, safety and treatment planning.
It becomes harmful when it communicates indifference, closes inquiry prematurely or prevents the patient from conveying essential information.
Conclusion
Patients deserve sufficient space to tell their stories. The spontaneous narrative is not an inconvenience; it is a central part of psychiatric assessment.
But psychiatric interviewing cannot remain entirely unstructured.
The psychiatrist must sometimes interrupt to:
- Establish chronology
- Clarify terminology
- Differentiate symptoms
- Return to unanswered questions
- Explore diagnostic alternatives
- Evaluate risk
- Protect the limited consultation from becoming clinically unfocused
An uninterrupted history may feel validating but still leave major diagnostic questions unresolved. A highly structured interview may obtain facts but fail to understand the person.
Good psychiatry requires both.
The most effective psychiatrist listens deeply, interrupts thoughtfully, redirects respectfully and explains clearly.
The purpose of interruption should never be to silence the patient.
It should be to ensure that the patient’s story becomes sufficiently clear to guide safe, accurate and meaningful treatment.
About the Author
Dr. Srinivas Rajkumar T
MD Psychiatry, AIIMS New Delhi
Senior Consultant Psychiatrist
Mind & Memory Clinic, Apollo Clinic Velachery, Chennai
Opposite Phoenix Marketcity
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
Related posts:
- Wu Wei: Zen for Psychiatrists — A Framework for Non-Forcing Clinical Practice
- Telemedicine Practice Guidelines 2020: A Simplified Guide for Psychiatrists
- Comprehensive Clinical Guide: Safe Antidepressant Discontinuation for Psychiatrists
- ICD-11 Personality Disorders: What Has Changed and Why It Matters in Clinical Practice
- Lorazepam-Assisted Interview: A Modern Substitute for Hypnosis in Clinical Practice
- Opioid Dose Equivalents in Clinical Practice: Bridging Heroin Use to Buprenorphine-Based OST