DSM-5 Conceptualisation of Autism Spectrum Disorder: A Clinical Perspective
 Autism Spectrum Disorder (ASD) represents a fundamental shift in psychiatric thinking—from rigid diagnostic categories to a dimensional, spectrum-based neurodevelopmental model.
Autism Spectrum Disorder (ASD) represents a fundamental shift in psychiatric thinking—from rigid diagnostic categories to a dimensional, spectrum-based neurodevelopmental model.
Both the DSM-5 and the ICD-11 converge on this understanding, though with subtle conceptual and clinical differences that are important in practice.
1. DSM-5: The Spectrum Model
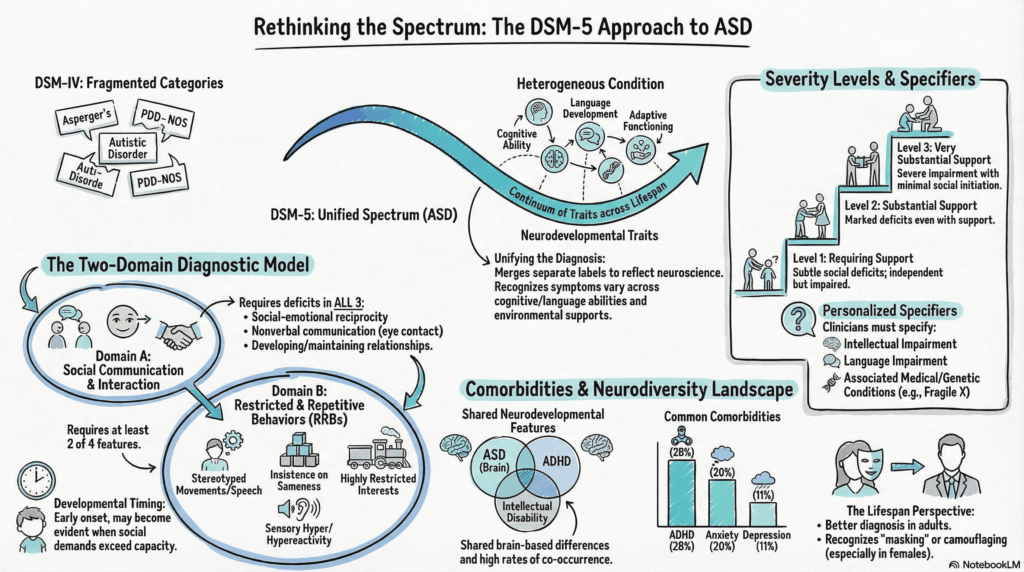
DSM-5 unified previously separate conditions (Autistic Disorder, Asperger’s, PDD-NOS) into a single spectrum, recognising:
- Clinical heterogeneity
- Shared neurodevelopmental mechanisms
- Variable functional impact
ASD is conceptualised as a disorder of:
- Social cognition and communication
- Behavioural flexibility and sensory processing
This aligns with evidence that ASD is a heterogeneous condition with diverse presentations across cognition, language, and environment .
2. Core DSM-5 Diagnostic Structure
Two Domains
A. Social Communication & Interaction (all required)
B. Restricted, Repetitive Behaviours (≥2 required)
Plus:
- Early developmental onset
- Functional impairment
- Exclusion of alternative explanations
3. ICD-11 Conceptualisation of ASD
The ICD-11 Autism Spectrum Disorder retains a similar core structure but differs in emphasis.
Key Features of ICD-11:
- Single diagnosis: Autism Spectrum Disorder (6A02)
- Subclassification based on:
- Intellectual development
- Functional language level
Examples:
- ASD with intellectual impairment and absent language
- ASD without intellectual impairment and with mild/no language impairment
4. DSM-5 vs ICD-11: Key Differences
A. Structural Approach
| Feature | DSM-5 | ICD-11 |
|---|---|---|
| Diagnostic Model | Spectrum + severity levels | Spectrum + functional subtypes |
| Domains | Explicit 2-domain model | Similar but less rigidly separated |
| Severity | Levels 1–3 (support-based) | Not explicitly tiered |
B. Severity vs Function
- DSM-5 → Severity Levels (Support-based)
- Focus: How much help does this person need?
- ICD-11 → Functional Descriptors
- Focus: What is the individual’s cognitive and language profile?
👉 Clinically:
- DSM-5 is more useful for treatment planning
- ICD-11 is often clearer for epidemiology and global coding
C. Language and Intellectual Profiling
ICD-11 gives greater emphasis to:
- Language ability
- Intellectual functioning
DSM-5 includes these as specifiers, but not as primary subclassifiers.
D. Social (Pragmatic) Communication Disorder
- DSM-5: Includes this as a separate diagnosis
- ICD-11: Less prominently separated
This difference becomes important in borderline or subthreshold presentations.
5. Convergence Between DSM-5 and ICD-11
Despite differences, both systems agree on:
- ASD as a neurodevelopmental condition
- Core deficits in:
- Social communication
- Behavioural flexibility
- Early developmental origin
- Frequent comorbidities:
- ADHD
- Anxiety
- Depression
6. Clinical Integration: How to Use Both Systems
In real-world practice:
DSM-5 helps you:
- Understand symptom clusters
- Assess severity
- Plan intervention intensity
ICD-11 helps you:
- Communicate functional profile
- Code for health systems
- Align with global standards
7. A Clinician’s Working Model
Integrating both systems, ASD can be conceptualised as:
A neurodevelopmental condition characterised by differences in social cognition, cognitive flexibility, and sensory processing, expressed across a spectrum and shaped by language, intelligence, and environmental supports.
8. Why This Matters Clinically
This dual-framework approach allows us to:
- Move beyond labels → toward individual profiles
- Recognise strengths alongside difficulties
- Tailor:
- Behavioural interventions
- Educational planning
- Pharmacological support for comorbidities
Conclusion
DSM-5 and ICD-11 together provide a complementary framework:
- DSM-5 → depth and clinical nuance
- ICD-11 → structure and global applicability
Understanding both allows for a more precise, personalised, and context-sensitive approach to autism.
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
With a clinical approach that integrates structured diagnostic frameworks, neurodevelopmental understanding, and technology-assisted assessments, Dr. Srinivas focuses on:
- Comprehensive ASD and ADHD evaluations
- QEEG-based brain mapping and neurofeedback
- Evidence-based behavioural and cognitive interventions
📩 srinivasaiims@gmail.com 📞 +91-8595155808