When Should Dementia Medicines Be Stopped?
Why MoCA Cut-Offs Help, But Should Never Be the Only Decision-Maker
One of the commonest questions families ask in dementia care is:
“Doctor, the memory has worsened despite medicines. Should we continue them?”
This is a very important question.
Dementia medicines are often started with hope. Families expect improvement in memory, behaviour, independence, and day-to-day functioning. But dementia is usually progressive. Over time, even with treatment, memory may decline, dependence may increase, and families may wonder whether the medicine is still helping.
The answer is not simple.
Dementia medicines should not be continued blindly. But they should also not be stopped casually. The right approach is to review the person as a whole — cognition, function, behaviour, medical health, side effects, stage of dementia, caregiver goals, and quality of life.
A MoCA score can guide us. But a MoCA score alone should never decide whether dementia medicines are stopped.
Which Dementia Medicines Are We Talking About?
When we say “dementia medicines,” we usually mean two major groups.
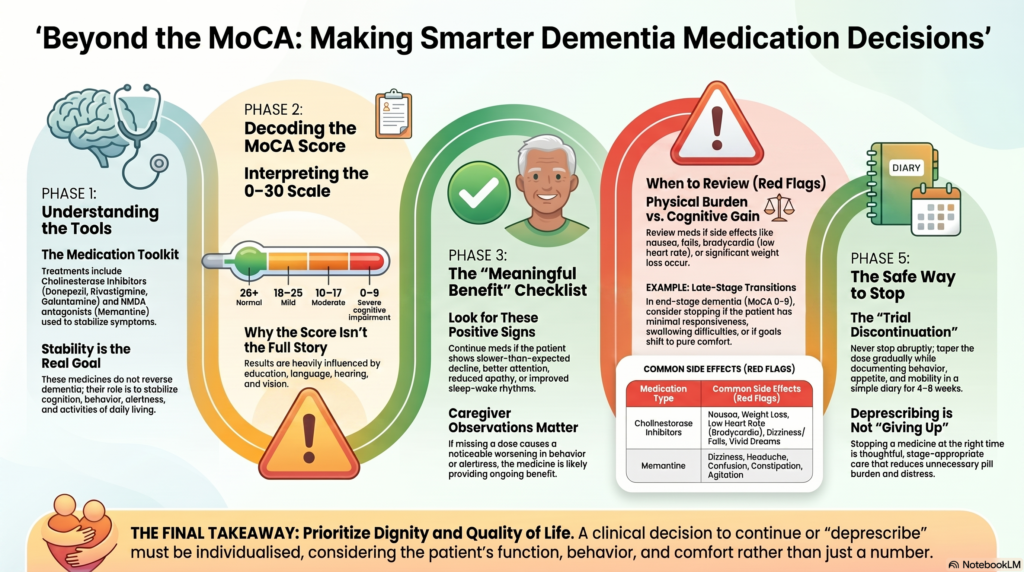
The first group is cholinesterase inhibitors:
- Donepezil
- Rivastigmine
- Galantamine
These medicines are commonly used in Alzheimer’s disease and may also be used in Lewy body dementia, Parkinson’s disease dementia, vascular dementia, or mixed dementia depending on the clinical situation.
The second medicine is memantine, an NMDA receptor antagonist. It is often used in moderate to severe Alzheimer’s disease and sometimes in combination with a cholinesterase inhibitor.
These medicines are not cures. They do not reverse dementia. They do not reliably stop the disease from progressing.
Their role is more modest but still meaningful: they may help stabilise cognition, behaviour, alertness, activities of daily living, or caregiver burden in some patients.
That is why the real question is not, “Is the memory normal now?”
The real question is:
“Is the patient doing better than expected, more stable than expected, or behaviourally easier to care for because of the medicine?”
Why Families Feel the Medicine Is “Not Working”
A common misunderstanding is that if the patient declines, the medicine has failed.
But dementia medicines do not usually produce dramatic improvement. Many times, the benefit is subtle:
- Slower decline
- Better attention
- Reduced apathy
- Better engagement
- Less agitation
- More stable sleep-wake rhythm
- Easier caregiving
- Slight preservation of daily functioning
- Fewer behavioural crises
Families may not notice this benefit until the medicine is stopped and the patient suddenly worsens.
This is why stopping should usually be a trial discontinuation, not a permanent decision made in one visit.
MoCA Cut-Offs: What Do the Scores Mean?
The Montreal Cognitive Assessment, or MoCA, is a widely used cognitive screening tool scored out of 30.
A practical interpretation is:
| MoCA Score | Usual Interpretation |
|---|---|
| 26 and above | Normal cognitive performance |
| 18–25 | Mild cognitive impairment range |
| 10–17 | Moderate cognitive impairment range |
| 0–9 | Severe cognitive impairment range |
A score around 18 is often used as a rough point where mild cognitive impairment and early Alzheimer-type dementia may overlap. But there is no perfect boundary. Dementia is not diagnosed by a number alone. Dementia requires cognitive decline plus loss of independence in daily life.
So, a person with MoCA 17 who is still managing daily affairs with support may be very different from another person with MoCA 17 who cannot manage medicines, money, cooking, hygiene, or travel.
The score is useful. But the story is more important.
Why MoCA Should Not Be Used Alone to Stop Medicines
Stopping dementia medicines purely because the MoCA has become low is a mistake.
There are several reasons.
First, MoCA is affected by education. People with fewer years of formal education may score lower even when the clinical severity is not as advanced.
Second, MoCA is affected by language. A person tested in a language they are not comfortable with may appear more impaired than they actually are.
Third, MoCA is affected by hearing, vision, hand function, tremor, stroke deficits, depression, anxiety, sleep deprivation, delirium, and poor cooperation.
Fourth, in advanced dementia, MoCA may show a floor effect. Once the score is very low, it becomes less useful for tracking meaningful change. At that stage, function and behaviour matter more than the test score.
Fifth, dementia medicines may help behaviour and function even when cognitive test scores remain low.
Therefore, the MoCA should be treated as one part of the decision, not the whole decision.
The Correct Question: Is There Meaningful Benefit?
Before stopping dementia medicines, we should ask:
- Has cognition clearly improved or stabilised after starting treatment?
- Has function declined more slowly than expected?
- Has the patient remained more alert or engaged?
- Are behavioural symptoms better controlled?
- Has caregiver burden reduced?
- Did stopping or missing doses previously worsen the patient?
- Are there side effects?
- Is the patient now in severe or end-stage dementia?
- Is the goal still preservation of function, or has the goal shifted to comfort?
A medicine may still be worth continuing even if memory is poor, especially if it helps behaviour, alertness, or daily care.
When Should Dementia Medicines Be Continued?
Dementia medicines should usually be continued when there is evidence of ongoing benefit.
Examples include:
1. The patient is stable
If the patient has not declined much over months, this may itself be a benefit. Stability in dementia is valuable.
2. Behaviour is better
In Lewy body dementia, Parkinson’s disease dementia, and some Alzheimer’s cases, cholinesterase inhibitors may help hallucinations, apathy, anxiety, agitation, or fluctuations. Stopping suddenly may worsen behaviour.
3. Daily functioning is preserved
If the patient is still able to dress, feed, communicate, move around, participate in routines, or recognise family better while on medicine, continuation may be reasonable.
4. Side effects are minimal
If the medicine is well tolerated and not creating medical complications, there may be no urgency to stop.
5. Caregiver reports clear worsening when doses are missed
This is an important real-world clue. If missing the medicine worsens alertness, behaviour, or sleep, it suggests some continuing benefit.
When Should Dementia Medicines Be Reviewed for Stopping?
A review is needed when the balance of benefit and burden changes.
The following situations should trigger a deprescribing discussion.
1. No Clear Benefit After an Adequate Trial
If the patient has taken the medicine regularly for several months and there has been no improvement, no stabilisation, and no reduction in rate of decline, it is reasonable to question whether the medicine is helping.
This does not mean stopping immediately in every case. But it means the family and clinician should discuss a supervised trial of discontinuation.
The key phrase is no meaningful benefit.
Meaningful benefit may include cognition, behaviour, daily function, alertness, or caregiver burden — not memory score alone.
2. Significant Decline Despite Treatment
If cognition and function have significantly worsened despite treatment, especially over the previous six months, continuing the same medicine indefinitely may not be useful.
However, this must be interpreted carefully.
A decline may be due to:
- Disease progression
- Delirium
- Infection
- Depression
- Sleep disorder
- Medication side effects from other drugs
- Stroke
- Metabolic problems
- Pain
- Sensory impairment
- Caregiver changes
- Environmental disruption
Before stopping dementia medicine, reversible causes of decline should be checked.
In dementia, sudden worsening is not always dementia progression. It is often delirium until proven otherwise.
3. Severe or End-Stage Dementia
Dementia medicines may be reviewed for stopping when the person reaches severe or end-stage dementia.
This is not decided by MoCA alone.
Severe or end-stage dementia usually means:
- Dependence in most or all activities of daily living
- Inability to dress, bathe, toilet, or feed independently
- Minimal meaningful communication
- Limited response to surroundings
- Bedbound or chair-bound state
- Recurrent aspiration, infections, or hospitalisations
- Difficulty swallowing medicines
- Weight loss or frailty
- Limited life expectancy
- Goals of care shifting from preservation to comfort
In this stage, the burden of continuing medicines may outweigh benefit. If the person can no longer meaningfully interact, swallow safely, or benefit functionally, stopping may be appropriate.
But even here, the decision should be individualised. Some patients worsen behaviourally when medicines are stopped. So, a monitored trial is better than abrupt discontinuation.
4. Troublesome Side Effects
Dementia medicines can cause side effects, especially in frail older adults.
Cholinesterase inhibitors may cause:
- Nausea
- Vomiting
- Loose stools
- Poor appetite
- Weight loss
- Dizziness
- Bradycardia
- Syncope
- Falls
- Sleep disturbance
- Vivid dreams
- Increased urinary frequency
- Worsening tremor in some patients
Memantine may cause:
- Dizziness
- Headache
- Confusion
- Constipation
- Sleepiness
- Agitation in some patients
Side effects matter more in older adults because even a “minor” side effect can lead to major consequences.
For example, dizziness may lead to a fall. Poor appetite may worsen frailty. Bradycardia may cause fainting. Diarrhoea may worsen dehydration. Sleep disturbance may worsen caregiver burden.
If the medicine is causing harm, stopping becomes more justified.
5. Cardiac Risk: Bradycardia, Syncope, Falls
This deserves special attention.
Cholinesterase inhibitors can reduce heart rate in susceptible patients. In an older adult with conduction problems, bradycardia, recurrent fainting, or unexplained falls, the dementia medicine should be reviewed.
This is especially important if the patient is also taking medicines such as beta-blockers, some calcium channel blockers, digoxin, or other drugs affecting heart rate.
A dementia medicine that slightly helps memory but increases falls may not be worth continuing.
A fractured hip can permanently worsen independence.
6. Weight Loss and Frailty
Weight loss is a very practical reason to reconsider cholinesterase inhibitors.
In dementia, nutrition is already fragile. If a patient loses appetite, becomes nauseous, develops diarrhoea, or loses weight after starting or increasing a cholinesterase inhibitor, the medicine should be reviewed.
In advanced dementia, preserving comfort, nutrition, and dignity may become more important than chasing small cognitive benefits.
7. Swallowing Difficulty or Pill Burden
In late-stage dementia, swallowing tablets may become difficult. The patient may pocket tablets, spit them out, cough, choke, or resist administration.
At this point, every medicine should be reviewed.
The question becomes:
Is this tablet still improving quality of life, or is it only adding distress?
If taking the medicine itself has become a daily battle, stopping may be reasonable.
Rivastigmine patch may be an option in some cases, but even patches can cause skin reactions, cost burden, and caregiver workload.
8. Poor Adherence or Medication Refusal
If the patient frequently refuses the medicine, misses doses, or becomes agitated during administration, the treatment burden may exceed benefit.
Forcing medicines in dementia can damage trust and increase behavioural symptoms. Medication plans must remain humane.
9. Limited Life Expectancy or Palliative Goals
When dementia reaches a palliative stage, the goal changes.
Earlier, the goal may be to preserve cognition and function. Later, the goal may be comfort, dignity, sleep, nutrition, pain control, and caregiver support.
In palliative care, medicines that do not provide clear comfort or short-term benefit should be reviewed.
Dementia medicines often have delayed, modest, and uncertain benefit. If life expectancy is limited, continuing them may not make sense unless they clearly help behaviour or comfort.
10. Wrong Indication
Sometimes dementia medicines are started for mild forgetfulness without a clear diagnosis of dementia.
For mild cognitive impairment, cholinesterase inhibitors are generally not routinely useful. If a person does not have a dementia syndrome and was started on these medicines without a clear indication, stopping should be considered.
The diagnosis should be reviewed carefully.
Not all memory complaints are dementia.
Depression, anxiety, poor sleep, thyroid problems, B12 deficiency, hearing loss, alcohol use, medication side effects, and stress can all mimic cognitive decline.
A Practical MoCA-Based Framework
MoCA can help structure the conversation, but it should not dictate the decision.
MoCA 18–25: Mild Impairment Range
At this stage, stopping dementia medicine is usually not based on the score alone.
If the patient has diagnosed dementia and is functioning relatively well, the focus should be on:
- Confirming diagnosis
- Monitoring progression
- Treating vascular risk factors
- Cognitive stimulation
- Exercise
- Sleep optimisation
- Hearing and vision correction
- Depression and anxiety treatment
- Medication adherence
- Caregiver education
If medicines were started appropriately and tolerated well, they are usually continued.
But if the diagnosis is actually mild cognitive impairment without functional loss, the need for dementia medicine should be reviewed.
MoCA 10–17: Moderate Impairment Range
This is often the stage where dementia medicines may be most actively considered.
Many patients in this range still have meaningful interaction, daily routines, behavioural symptoms, and caregiver-dependent functioning.
Stopping purely because the score is in the moderate range is usually not appropriate.
Instead, ask:
- Is there stabilisation?
- Is behaviour better?
- Is the patient more alert?
- Are activities of daily living better preserved?
- Are side effects acceptable?
- Is caregiver burden reduced?
If yes, continuing may be reasonable.
MoCA 0–9: Severe Impairment Range
This is the stage where stopping may be more seriously discussed.
But even here, the decision should not be automatic.
A patient with MoCA 8 who still walks, eats, smiles, interacts, participates in routines, and has fewer hallucinations on medicine may still benefit.
A patient with MoCA 3 who is bedbound, barely responsive, losing weight, choking on tablets, and fully dependent may not benefit meaningfully.
Therefore, in MoCA 0–9, the decision should be driven mainly by:
- Functional dependence
- Responsiveness
- Behavioural stability
- Comfort
- Swallowing ability
- Frailty
- Side effects
- Goals of care
- Caregiver observations
The number opens the discussion. It does not close the decision.
How to Stop Dementia Medicines Safely
Stopping should usually be done gradually.
A practical approach is:
- Discuss goals with family and caregivers.
- Document baseline cognition, function, behaviour, sleep, appetite, mobility, and caregiver burden.
- Stop one medicine at a time.
- Taper rather than abruptly stop, unless there is a serious adverse effect.
- Monitor every few weeks.
- Restart if there is clear deterioration after stopping and no other explanation.
For example, the dose may be reduced stepwise over several weeks. After each reduction, the family should watch for:
- Sudden worsening of confusion
- Increased agitation
- New hallucinations
- Sleep disruption
- Reduced communication
- Decline in feeding
- Decline in mobility
- Increased caregiver difficulty
If there is clear worsening after stopping, and no infection, delirium, medication change, or environmental cause is found, restarting may be appropriate.
Deprescribing should not be seen as “giving up.” It is a monitored clinical trial.
What Should Families Monitor After Stopping?
Families should keep a simple diary for four to eight weeks.
Track:
- Sleep
- Appetite
- Communication
- Recognition
- Agitation
- Hallucinations
- Wandering
- Toileting
- Feeding
- Mobility
- Falls
- Caregiver burden
- New confusion
- Emotional distress
The most important question is:
“Is the person clearly worse after stopping?”
If yes, the medicine may have been providing benefit.
If no, stopping may reduce pill burden without harm.
When Not to Stop Casually
There are situations where stopping needs extra caution.
Lewy Body Dementia and Parkinson’s Disease Dementia
In these conditions, cholinesterase inhibitors may help hallucinations, fluctuations, attention, and behaviour. Stopping may worsen neuropsychiatric symptoms in some patients.
Previous Clear Benefit
If the family says the patient clearly improved after starting the medicine, stopping should be cautious.
Severe Behavioural Symptoms
If the medicine appears to reduce hallucinations, agitation, aggression, or distress, continuation may be justified even with low cognitive scores.
Recent Delirium or Medical Illness
Do not stop during an acute illness unless the medicine itself is causing harm. Wait until the patient is medically stable, otherwise decline may be wrongly attributed to stopping.
Common Mistakes in Stopping Dementia Medicines
Mistake 1: Stopping only because memory worsened
Dementia can worsen despite treatment. The question is whether the decline is slower or behaviour is better.
Mistake 2: Using MoCA as the only criterion
MoCA is a screening tool, not a complete clinical decision-maker.
Mistake 3: Abruptly stopping without monitoring
Sudden discontinuation may sometimes worsen cognition, function, or behaviour.
Mistake 4: Stopping during infection or delirium
Acute confusion should first be evaluated medically.
Mistake 5: Ignoring caregiver observations
Caregivers often detect meaningful changes better than test scores.
Mistake 6: Continuing forever without review
Long-term medicines should be reviewed periodically. “Started once, continued forever” is not good dementia care.
A Balanced Clinical Rule
A useful rule is:
Continue dementia medicines when there is meaningful benefit and tolerable risk.
Consider stopping when there is no meaningful benefit, significant side effect burden, severe/end-stage dementia, limited life expectancy, swallowing difficulty, or goals of care have shifted to comfort.
Do not stop based on MoCA alone.
The Final Takeaway
Dementia medicines are not miracle drugs, but they are not useless either.
For some patients, they provide meaningful stabilisation. For others, they add side effects, pill burden, cost, and distress without clear benefit.
The decision to stop should be individualised.
MoCA cut-offs can guide staging:
- 26 and above: normal cognitive performance
- 18–25: mild impairment
- 10–17: moderate impairment
- 0–9: severe impairment
But the most important clinical questions are:
- Is the patient functioning better or more stable because of the medicine?
- Are behavioural symptoms controlled?
- Are side effects present?
- Is the patient still able to benefit meaningfully?
- What are the family’s goals now — preservation, stability, comfort, or palliation?
In dementia care, good prescribing matters. Good deprescribing matters just as much.
Stopping a medicine at the right time is not abandonment. It is thoughtful, humane, stage-appropriate care.
Need Help With Dementia Assessment and Care Planning?
Dementia care requires more than writing a prescription. A proper plan should include diagnosis, cognitive staging, functional assessment, behavioural symptom management, caregiver counselling, home safety, medication review, and long-term planning.
I provide structured assessment and treatment planning for memory problems, mild cognitive impairment, dementia, behavioural and psychological symptoms of dementia, caregiver stress, and medication review.
If you are unsure whether dementia medicines should be started, continued, changed, or stopped, a detailed clinical review can help the family make a safer and more confident decision.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Apollo Clinic Velachery, Chennai
Opp. Phoenix Mall
Email: srinivasaiims@gmail.com
Phone: +91-8595155808
The goal is not just to treat memory scores. The goal is to preserve dignity, reduce suffering, support families, and improve quality of life at every stage of dementia.