Lithium vs Valproate: A Comprehensive, Clinically Grounded Guide to Decision-Making in Bipolar Disorder
 The choice between Lithium and Valproate is not merely pharmacological—it is conceptual, longitudinal, and patient-specific. Both are called “mood stabilizers,” yet they represent fundamentally different approaches to bipolar illness.
The choice between Lithium and Valproate is not merely pharmacological—it is conceptual, longitudinal, and patient-specific. Both are called “mood stabilizers,” yet they represent fundamentally different approaches to bipolar illness.
A thoughtful clinician does not ask “Which is better?” but rather:
“Which drug best matches the patient’s illness trajectory, biology, and psychosocial context?”
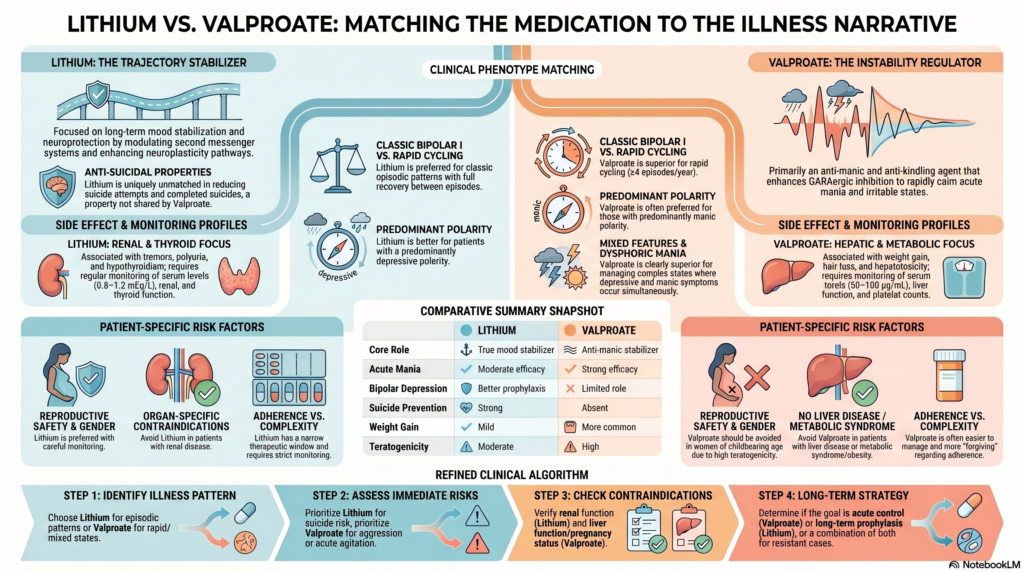
1. Two Different Philosophies of Treatment
Lithium
- A true mood stabilizer
- Works across mania, depression, and maintenance
- Has anti-suicidal and neuroprotective properties
👉 Think:
Trajectory stabilizer
Valproate
- Primarily an anti-manic, anti-kindling agent
- Strong in acute control and unstable mood states
- Less robust for depressive prevention
👉 Think:
Instability regulator
2. Mechanistic Foundations (Why They Differ Clinically)
Lithium
- Modulates second messenger systems (IP3, cAMP)
- Inhibits GSK-3β
- Enhances neuroplasticity (BDNF pathways)
👉 Leads to:
- Long-term mood stabilization
- Reduced recurrence
- Unique anti-suicidal effect
Valproate
- Enhances GABAergic inhibition
- Reduces neuronal excitability
- Acts as an anti-kindling agent
👉 Leads to:
- Rapid calming of mania
- Better control of mixed and irritable states
3. Clinical Phenotype-Based Decision Making
A. Classic Bipolar I (Episodic Pattern)
- Clear manic and depressive episodes
- Full inter-episode recovery
→ Lithium preferred
B. Rapid Cycling Bipolar Disorder
- ≥4 episodes/year
- Unstable course
→ Valproate preferred
C. Mixed Features / Dysphoric Mania
- Simultaneous depressive + manic symptoms
→ Valproate clearly superior
D. Predominantly Depressive Polarity
→ Lithium preferred
- Better prophylaxis for depression
E. Predominantly Manic Polarity
→ Valproate often preferred
4. Course and Longitudinal Thinking
| Illness Pattern | Best Fit |
|---|---|
| Episodic, stable between episodes | Lithium |
| Chronic, fluctuating, unstable | Valproate |
| Progressive “kindling” pattern | Valproate |
5. Suicide Risk: A Decisive Factor
→ Lithium is unmatched
- Reduces:
- Suicide attempts
- Completed suicides
👉 If suicidality is central:
Lithium should strongly be considered unless contraindicated
6. Acute vs Maintenance Strategy
Acute Mania
- Severe agitation, irritability → Valproate (faster onset)
Maintenance
- Prevent recurrence → Lithium (gold standard)
👉 In practice:
- Start with Valproate for control
- Transition or combine with Lithium for stability
7. Patient-Specific Decision Factors
A. Gender and Reproductive Risk
Women of childbearing age:
- Avoid Valproate (high teratogenicity)
- Prefer Lithium (with monitoring)
B. Medical Comorbidities
| Condition | Avoid | Prefer |
|---|---|---|
| Renal disease | Lithium | Valproate |
| Liver disease | Valproate | Lithium |
| Obesity/metabolic syndrome | Valproate | Lithium |
C. Cognitive and Functional Profile
- Lithium → mild cognitive dulling (dose-dependent)
- Valproate → sedation, attentional slowing
D. Adherence and Practicality
- Lithium:
- Narrow therapeutic window
- Requires regular monitoring
- Valproate:
- Easier to manage
- More forgiving
👉 Poor adherence → Valproate may be more practical
8. Side Effect Profiles
Lithium
- Tremor
- Polyuria (DI-like state)
- Hypothyroidism
- Long-term renal concerns
Valproate
- Weight gain
- Sedation
- Hair loss
- Hepatotoxicity
- Thrombocytopenia
- Strong teratogenic risk
9. Monitoring Requirements
Lithium
- Serum levels (0.6–1.2 mEq/L)
- Renal function
- Thyroid function
Valproate
- Serum levels (50–100 µg/mL)
- Liver function
- Platelet counts
10. Special Clinical Situations
| Scenario | Preferred Approach |
|---|---|
| Severe agitation/aggression | Valproate |
| High suicide risk | Lithium |
| Comorbid substance use | Valproate |
| Elderly patient | Valproate (often better tolerated) |
| Psychotic features | Add antipsychotic (both need augmentation) |
11. Combination Therapy
In resistant or severe cases:
- Lithium + Valproate
Rationale:
- Complementary mechanisms
- Broader coverage of mood spectrum
12. Final Comparative Summary Table
| Domain | Lithium | Valproate |
|---|---|---|
| Core role | True mood stabilizer | Anti-manic stabilizer |
| Best phenotype | Classic Bipolar I | Rapid cycling, mixed states |
| Acute mania | Moderate | Strong |
| Bipolar depression | Better | Limited |
| Maintenance | Gold standard | Selective role |
| Suicide prevention | Strong | Absent |
| Course pattern | Episodic | Chronic/unstable |
| Agitation | Limited | Strong |
| Weight gain | Mild | More common |
| Renal risk | Yes | No |
| Hepatic risk | No | Yes |
| Teratogenicity | Moderate | High |
| Monitoring | Strict | Moderate |
| Adherence ease | Lower | Higher |
13. A Refined Clinical Algorithm
Step 1: Identify illness pattern
- Episodic → Lithium
- Rapid/mixed → Valproate
Step 2: Assess risk
- Suicide → Lithium
- Aggression/instability → Valproate
Step 3: Check contraindications
- Renal → avoid Lithium
- Liver/pregnancy → avoid Valproate
Step 4: Think longitudinally
- Acute control vs long-term stability
14. The Deeper Clinical Insight
This decision reflects two fundamentally different therapeutic orientations:
-
Lithium
Stabilizes the illness across time
-
Valproate
Stabilizes the illness in the moment
The most effective treatment strategies often integrate both perspectives.
Conclusion
Lithium and Valproate are not competitors—they are complementary tools.
- Choose Lithium when:
- You are thinking long-term, prophylaxis, and suicide prevention
- Choose Valproate when:
- You are managing instability, agitation, or complex mood patterns
Ultimately:
Good psychiatry is not about choosing a drug—it is about matching a drug to the narrative of the illness.
For Clinical Practice & Consultation
For complex bipolar disorder, treatment resistance, or nuanced medication planning, a structured, individualized approach can significantly improve patient outcomes.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Senior Consultant Psychiatrist
Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808