Steady State & Drug Level Monitoring in Psychiatry: A Practical Guide (Lithium & Valproate)
 In psychopharmacology, prescribing a drug is only half the job. The other half is knowing when the drug has reached a stable level in the body—and whether that level is therapeutic, subtherapeutic, or toxic. This is the essence of steady state and therapeutic drug monitoring (TDM)—especially critical for drugs like Lithium and Valproate.
In psychopharmacology, prescribing a drug is only half the job. The other half is knowing when the drug has reached a stable level in the body—and whether that level is therapeutic, subtherapeutic, or toxic. This is the essence of steady state and therapeutic drug monitoring (TDM)—especially critical for drugs like Lithium and Valproate.
🔹 What is “Steady State”?
Steady state is the point at which:
The amount of drug entering the body equals the amount being eliminated
At this stage:
- Blood drug levels become stable (plateau)
- Fluctuations occur within a predictable range
- Measured levels reflect the true pharmacological effect
🔹 The Half-Life Rule (Core Concept)
Steady state is determined by a drug’s half-life (t½).
👉 Rule of thumb:
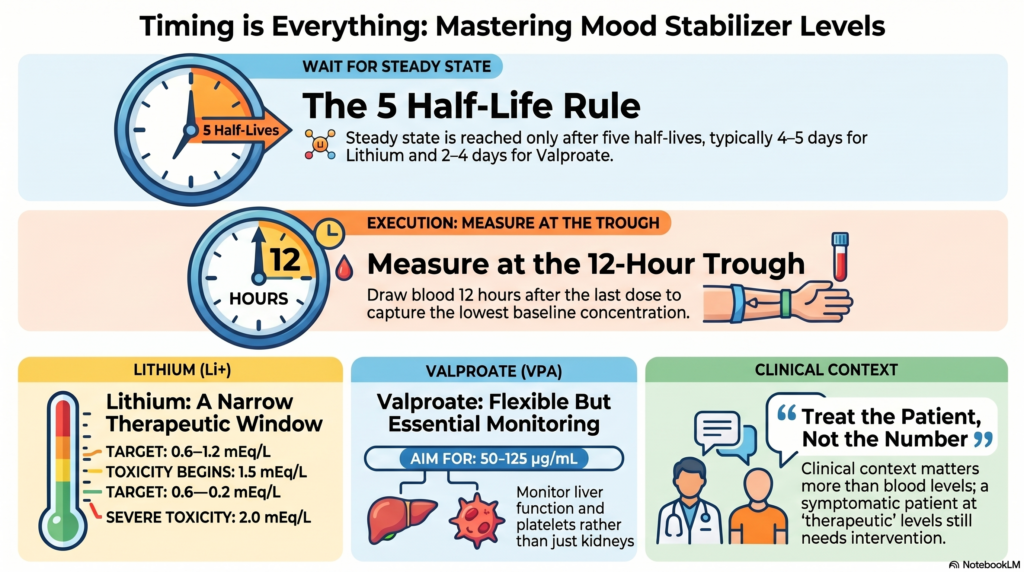
- Steady state is reached after ~5 half-lives
Example:
| Drug | Half-life | Steady state reached in |
|---|---|---|
| Lithium | ~18–24 hours | ~4–5 days |
| Valproate | ~9–16 hours | ~2–4 days |
👉 This is why:
- You don’t check levels too early
- Early levels can be misleading
🔹 Why Steady State Matters Clinically
If you measure drug levels before steady state:
- You may underestimate the true level
- Risk of unnecessary dose escalation
- Potential for toxicity later
👉 Correct timing ensures:
- Accurate dose adjustments
- Safer titration
- Better outcomes
🔹 What is Therapeutic Drug Monitoring (TDM)?
TDM involves:
Measuring drug concentration in blood to ensure it lies within a therapeutic window
Why TDM is crucial in psychiatry:
- Narrow therapeutic index (especially lithium)
- Variable metabolism between patients
- Risk of toxicity
- Non-adherence detection
🔹 Lithium: The Prototype Drug for Monitoring
🎯 Therapeutic Range:
| Phase | Serum Level |
|---|---|
| Acute mania | 0.8 – 1.2 mEq/L |
| Maintenance | 0.6 – 1.0 mEq/L |
⏱️ When to Check Levels?
👉 12-hour trough level (gold standard)
- Draw blood:
- 12 hours after last dose
- After 5 days of stable dosing
⚠️ Toxicity Levels:
- >1.5 mEq/L → Toxicity begins
- >2.0 mEq/L → Severe toxicity
🔍 Factors Affecting Lithium Levels:
- Renal function
- Dehydration
- Sodium balance
- Drug interactions (e.g., NSAIDs, ACE inhibitors)
🔹 Valproate: Flexible but Still Needs Monitoring
🎯 Therapeutic Range:
| Indication | Level |
|---|---|
| Mania | 50 – 125 µg/mL |
| Epilepsy (reference) | ~50–100 µg/mL |
⏱️ When to Check Levels?
- After 3–5 days (steady state)
- Trough level preferred (just before next dose)
⚠️ Toxicity:
-
150 µg/mL → Increased risk
- Watch for:
- Sedation
- Tremor
- Hepatotoxicity
🔍 Special Considerations:
- High protein binding → free drug may vary
- Liver function matters
- Platelet counts may drop
🔹 Practical Clinical Scenarios
1. Early Testing Error
Patient on lithium for 2 days → level = 0.4
👉 Misleading → not at steady state
2. Sudden Toxicity
Stable lithium patient develops vomiting → level rises
👉 Likely dehydration → reduced clearance
3. “Therapeutic Level, Still Symptomatic”
Valproate level = 80, but mania persists
👉 Treat the patient, not just the number
🔹 The Concept of “Trough Level”
A trough level is:
The lowest concentration of drug in blood before the next dose
Why it matters:
- Reflects true steady state baseline
- Minimizes variability
- Standardizes interpretation
🔹 Key Differences: Lithium vs Valproate
| Feature | Lithium | Valproate |
|---|---|---|
| Monitoring necessity | Essential | Recommended |
| Therapeutic index | Narrow | Wider |
| Toxicity risk | High | Moderate |
| Organ affected | Kidney | Liver |
🔹 Common Mistakes to Avoid
❌ Checking levels before steady state
❌ Not standardizing timing (random sampling)
❌ Ignoring clinical context
❌ Over-relying on numbers
About the Author
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist
Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808
If you are looking for safe, evidence-based mood stabilizer management with monitoring, you can reach out for consultation.