What Changes First After Starting OCD Treatment?
 Many people who start treatment for OCD ask the same question: “Doctor, when will these thoughts stop?” It is a very natural question. OCD can be exhausting because the mind keeps producing doubts, fears, images, urges, or “what if” questions even when the person does not want them. A person may know that the thought is unreasonable, but still feel driven to check, wash, repeat, pray, confess, avoid, search online, or ask for reassurance.
Many people who start treatment for OCD ask the same question: “Doctor, when will these thoughts stop?” It is a very natural question. OCD can be exhausting because the mind keeps producing doubts, fears, images, urges, or “what if” questions even when the person does not want them. A person may know that the thought is unreasonable, but still feel driven to check, wash, repeat, pray, confess, avoid, search online, or ask for reassurance.
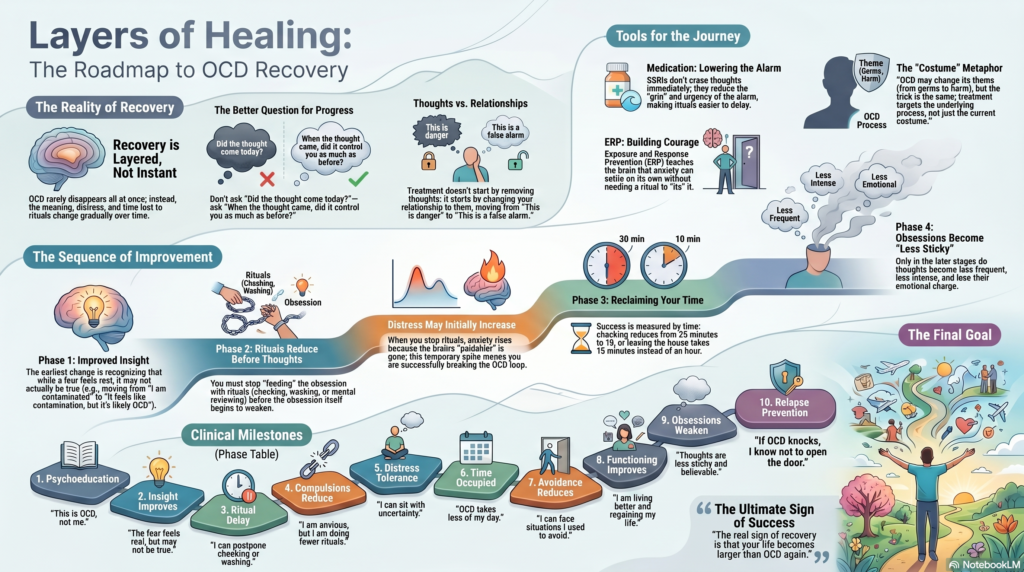
But OCD recovery usually does not happen by simply switching off thoughts. It happens more gradually. The first sign of improvement is often not that the thought disappears. The first sign is that the thought begins to lose its authority.
In the beginning, OCD may still speak loudly. But the person slowly begins to say, “This is OCD. This is a false alarm. I do not have to obey it.” This shift is important. Research shows that insight in OCD is not fixed; it can change over time, and improvement in insight is associated with improvement in OCD severity.
The first change is usually: “I recognise this as OCD”
Before treatment, the person may feel trapped inside the thought.
A contamination fear feels like real danger. A doubt about locking the door feels like a real possibility of disaster. A religious or sexual intrusive thought feels like proof of being immoral. A harm thought feels like a warning sign. A relationship doubt feels like something that must be solved immediately.
After treatment begins, the thought may still come, but the person starts seeing it differently.
Earlier, the mind said, “This is dangerous.”
Later, the person begins to say, “This feels dangerous because OCD is exaggerating the signal.”
Earlier, the thought demanded action.
Later, the person begins to create a pause between the thought and the ritual.
This pause is one of the earliest signs of recovery.
OCD is not measured only by the presence of thoughts. Standard clinical assessment also looks at time occupied, interference, distress, resistance, and control over obsessions and compulsions. So a patient may be improving even if intrusive thoughts are still present, provided they are spending less time on them, believing them less, resisting rituals better, and returning to normal life faster.
The next change: compulsions start reducing
Many patients feel disappointed when the thought continues after treatment begins. They may say, “The thought is still coming, so maybe I am not improving.” But in OCD, thoughts often reduce later. The compulsion usually needs to change first.
This is because OCD survives through a loop. A thought comes. The thought creates anxiety, guilt, disgust, fear, or uncertainty. The person performs a compulsion. The compulsion gives temporary relief. Because relief comes immediately, the brain learns that the compulsion was necessary. Next time the same doubt appears, the urge to ritualise becomes stronger.
This is why compulsions are so powerful. They help for a few minutes, but they strengthen OCD in the long run.
Compulsions are not only visible actions. Washing, checking, arranging, repeating, and cleaning are common, but many compulsions are hidden. Mental review, silent prayer, replacing “bad thoughts” with “good thoughts,” confession, repeated self-analysis, reassurance seeking, and internet searching can also function as compulsions.
Treatment begins to work when the patient learns to reduce these rituals. The first goal is not, “No thought should come.” The first goal is, “Even if the thought comes, I will not feed it with a ritual.”
This is the heart of exposure and response prevention, or ERP. ERP involves facing OCD triggers in a planned and graded way while resisting the compulsion that usually follows. The Indian Psychiatric Society guidelines describe ERP as a core component of CBT for OCD, along with psychoeducation, hierarchy building, cognitive restructuring, homework practice, and relapse prevention.
A simple way to understand this is:
Recovery begins when you stop obeying OCD, not when OCD stops talking.
Anxiety may initially rise before it falls
This is one of the most important things patients and families must understand.
When a person stops checking, washing, confessing, repeating, or asking for reassurance, anxiety may temporarily increase. This can feel frightening. The patient may think, “I tried not doing the ritual and I felt worse. So maybe treatment is not working.”
Actually, this may be the beginning of real recovery.
The brain is used to getting relief through rituals. When the ritual is blocked, the brain protests. The anxiety rises because OCD is not getting its usual safety behaviour. But if the person stays with the discomfort without doing the ritual, the brain slowly learns a new lesson: “Anxiety can rise and fall on its own. I do not need to perform the ritual to survive this feeling.”
This is why ERP is not simply about “facing fear.” It is about learning a new relationship with fear. The patient learns that uncertainty, discomfort, guilt, disgust, or “not just right” feelings can be tolerated without compulsions.
Over time, this creates a different kind of confidence. The patient may still feel anxious, but the anxiety no longer controls behaviour.
Then OCD starts taking less time from life
After insight improves and compulsions begin to reduce, the next visible improvement is often time.
The patient may still have the thought, but OCD occupies less of the day. A person who earlier spent one hour checking may reduce it to twenty minutes, then ten minutes, then one planned check. Someone who washed repeatedly may still feel contaminated, but the washing becomes shorter and less elaborate. Someone who asked reassurance twenty times may ask five times, then once, and later learn to tolerate the doubt without asking.
This reduction in time is a major clinical improvement. OCD is not just a disorder of thoughts; it is a disorder that steals time, freedom, confidence, relationships, and daily functioning.
A patient may say, “The thought came, but I moved on faster.” That is improvement.
Another may say, “I still felt anxious, but I went to work.” That is improvement.
Another may say, “I wanted to ask my family for reassurance, but I delayed it.” That is improvement.
Recovery is not measured only by a silent mind. It is measured by a freer life.
Functioning improves before complete symptom disappearance
As OCD takes less time, the patient’s life slowly expands again.
They may leave home faster. Bathing and dressing become easier. Work improves. Studies improve. Family arguments reduce. The person avoids fewer situations. They regain the ability to travel, cook, pray, touch objects, care for children, drive, read, or make decisions without being trapped in endless doubt.
This functional recovery is very important. Some patients continue to have occasional intrusive thoughts, but they are functioning much better. That is meaningful recovery.
OCD treatment should therefore focus not only on symptom reduction but also on restoring daily life. The guidelines emphasise regular work, normal behaviours, booster sessions, and preparation for future symptom changes or stress-related relapse.
A good way to explain this to patients is:
The goal is not to create a perfectly empty mind. The goal is to stop living according to OCD’s rules.
The thoughts usually become weaker later
Patients often expect thoughts to stop first. In reality, the thoughts often reduce later.
What changes first is the patient’s response. Then the time spent reduces. Then avoidance reduces. Then functioning improves. Over time, the thoughts themselves become less frequent, less sticky, less believable, and less emotionally charged.
Earlier, the thought felt like an emergency.
Later, it feels like an irritation.
Still later, it becomes background noise.
Eventually, the person may say, “The thought came, but I did not take it seriously.”
This is a major shift. OCD recovery is not always about never having intrusive thoughts. Everyone has strange, unwanted, or uncomfortable thoughts at times. The difference is that in OCD, the thought becomes meaningful, threatening, and urgent. Treatment helps remove that false meaning and urgency.
Why symptoms sometimes change shape during treatment
A common experience in OCD recovery is symptom shifting.
A patient may say, “My washing has reduced, but now I am checking more.”
Another may say, “My religious thoughts reduced, but now I have relationship doubts.”
Someone else may say, “Earlier I had visible rituals. Now I am doing mental rituals.”
This does not always mean the illness is worsening. OCD often changes its theme. The costume changes, but the mechanism remains the same.
The old theme may be contamination. The new theme may be harm. Then it may become morality, religion, sexuality, health, relationships, or perfectionism. But underneath, OCD is still using the same process: doubt, distress, neutralising, temporary relief, and more doubt.
This is why treatment should not chase only one theme. The real target is the OCD process itself.
A recent network analysis of OCD symptoms during ERP found that symptoms are interconnected. At baseline, symptoms clustered around resistance/control and interference/distress. With effective ERP, these symptom networks became more integrated, especially in patients who improved dramatically, suggesting that better control over obsessions and compulsions may go along with reduced distress and interference.
In simple terms, when one part of OCD loosens, other parts can begin to loosen too.
Recovery is not the same for every patient
Some patients improve quickly. Some improve gradually. Some show partial improvement and need treatment adjustment. Some patients initially improve and then plateau.
This is normal. OCD is heterogeneous.
In a large pooled study of adults receiving manualised ERP, researchers identified different treatment trajectories: some patients showed dramatic improvement, many showed moderate improvement, and a smaller group showed little-to-no progress. Avoidance and broader internalising symptoms predicted poorer progress.
This has an important clinical message. If a patient is not improving, it does not always mean they are “not trying” or that treatment has failed. We need to look carefully for hidden maintaining factors.
Is the patient still avoiding triggers? Are family members giving reassurance? Are mental rituals continuing? Is depression reducing motivation? Is insight poor? Are there tics, ADHD, autism traits, bipolarity, personality vulnerabilities, or another condition modifying the course? Is the patient doing ERP only in the clinic but not at home?
Good OCD care is not just prescribing medicine or giving advice. It requires careful formulation.
Medicines and therapy work differently, but can support each other
With medicines such as SSRIs, the first change may be subtle. The thought may feel less sticky. The urge to ritualise may reduce. Anxiety may become more tolerable. Sleep and mood may improve. The patient may find it easier to resist compulsions.
But OCD usually needs patience. Treatment guidelines commonly recommend an adequate SSRI trial of around 8–12 weeks to determine response, and OCD often requires higher anti-obsessional doses than those used for depression or general anxiety.
ERP works through behavioural learning. It teaches the brain that the feared situation can be faced without rituals. Medicines may reduce the intensity of the alarm. ERP teaches the person not to obey the alarm.
For many patients, the combination is powerful: medicine reduces the grip of OCD, and ERP builds freedom from OCD.
Mood often improves when OCD improves
Many people with OCD develop low mood because they feel trapped, ashamed, exhausted, or hopeless. They may lose time, confidence, relationships, productivity, and self-respect.
As OCD improves, mood often improves too. A six-year longitudinal study found that OCD symptom severity predicted later depression severity, while depression did not meaningfully predict later OCD severity in that sample. The authors suggested that treating OCD should usually be prioritised, while still monitoring depression and suicidal thoughts carefully.
This is clinically important. Depression should never be ignored, especially if there is hopelessness, suicidal thinking, poor self-care, or inability to participate in therapy. But in many patients, when OCD loses control over daily life, mood and confidence begin to return.
Relapse prevention is part of recovery
OCD can wax and wane. Stress, exams, illness, childbirth, job change, relationship stress, sleep deprivation, or family conflict can bring back symptoms. This does not mean treatment has failed.
A spike is not the same as relapse. A spike becomes relapse when the person returns to old rituals, avoidance, reassurance seeking, and fear-based living.
Patients should learn to identify early warning signs. For example, checking becomes “just once more.” Reassurance seeking quietly increases. Mental review returns. Avoidance expands. Internet searching increases. The family again starts participating in rituals. Old themes return or new themes appear.
Relapse prevention means recognising these early signs and returning to the treatment principles quickly: label it as OCD, reduce rituals, reduce avoidance, tolerate uncertainty, continue normal routine, and seek booster help when needed.
A reassuring message for patients
OCD recovery is not a straight line. It is more like retraining a sensitive alarm system.
At first, the alarm may still ring. But you learn that every alarm does not require action. Then you stop running to check every signal. Then the alarm rings less often. Then even when it rings, you do not panic. Eventually, your life becomes bigger than the alarm.
So, after starting OCD treatment, do not ask only, “Did the thought come?”
Ask better questions:
Did I believe it less?
Did I ritualise less?
Did I avoid less?
Did I spend less time?
Did I return to my day faster?
Did I live more freely despite the thought?
That is how OCD improves.
The thoughts often reduce last. What improves first is insight, ritual control, distress tolerance, time occupied, avoidance, and functioning.
OCD recovery is not about winning an argument with every thought. It is about learning that you do not have to answer every thought.
Need help for OCD?
OCD is treatable. With proper assessment, psychoeducation, CBT with ERP, appropriate medication when needed, family guidance, and relapse prevention, many people can regain control over their lives.
Dr. Srinivas Rajkumar T, MD (AIIMS, New Delhi), DNB, MBA (BITS Pilani)
Consultant Psychiatrist & Neurofeedback Specialist
Mind & Memory Clinic, Apollo Clinic Velachery (Opp. Phoenix Mall)
✉ srinivasaiims@gmail.com 📞 +91-8595155808